

Myocardial hypertrophy and its role in heart failure with preserved ejection fraction
- PMID: 26183480
- PMCID: PMC4652334
- DOI: 10.1152/japplphysiol.00374.2015
Myocardial hypertrophy and its role in heart failure with preserved ejection fraction
Abstract
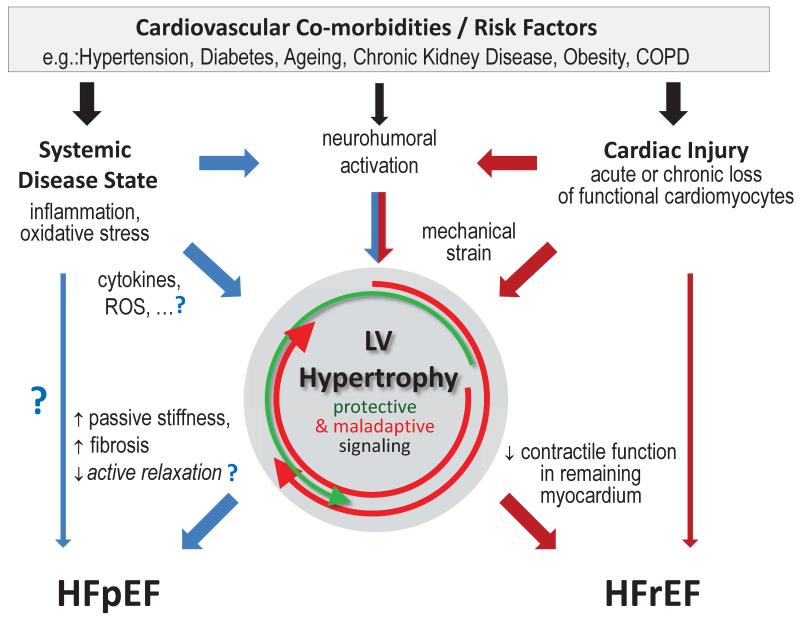
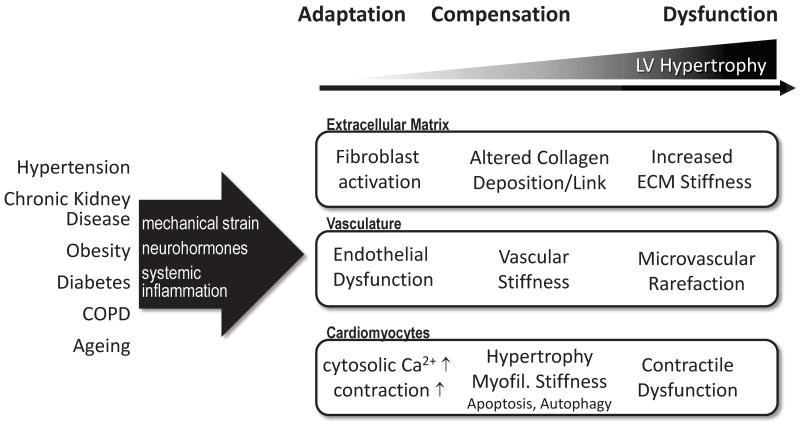
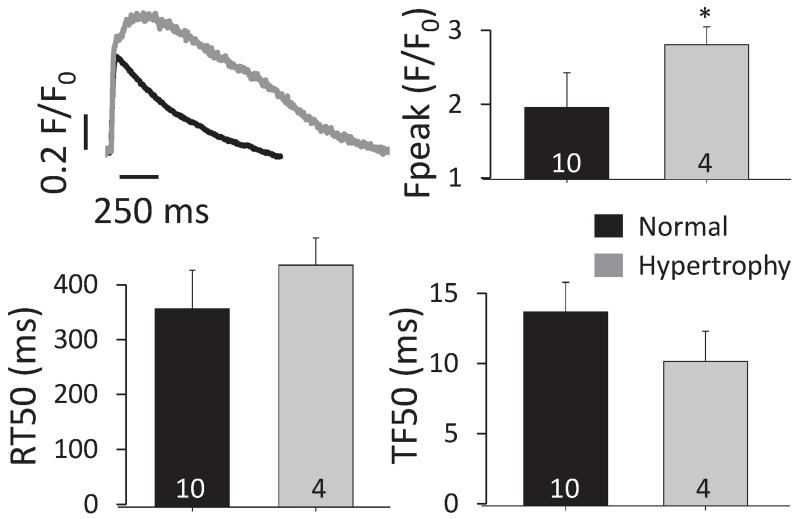
Left ventricular hypertrophy (LVH) is the most common myocardial structural abnormality associated with heart failure with preserved ejection fraction (HFpEF). LVH is driven by neurohumoral activation, increased mechanical load, and cytokines associated with arterial hypertension, chronic kidney disease, diabetes, and other comorbidities. Here we discuss the experimental and clinical evidence that links LVH to diastolic dysfunction and qualifies LVH as one diagnostic marker for HFpEF. Mechanisms leading to diastolic dysfunction in LVH are incompletely understood, but may include extracellular matrix changes, vascular dysfunction, as well as altered cardiomyocyte mechano-elastical properties. Beating cardiomyocytes from HFpEF patients have not yet been studied, but we and others have shown increased Ca(2+) turnover and impaired relaxation in cardiomyocytes from hypertrophied hearts. Structural myocardial remodeling can lead to heterogeneity in regional myocardial contractile function, which contributes to diastolic dysfunction in HFpEF. In the clinical setting of patients with compound comorbidities, diastolic dysfunction may occur independently of LVH. This may be one explanation why current approaches to reduce LVH have not been effective to improve symptoms and prognosis in HFpEF. Exercise training, on the other hand, in clinical trials improved exercise tolerance and diastolic function, but did not reduce LVH. Thus current clinical evidence does not support regression of LVH as a surrogate marker for (short-term) improvement of HFpEF.
Keywords: HFpEF; cardiac myocytes; diastolic dysfunction; left ventricular hypertrophy; remodeling.
Copyright © 2015 the American Physiological Society.
Figures
References
-
- Balogun MO, Dunn FG. Systolic and diastolic function following regression of left ventricular hypertrophy in hypertension. J Hypertens Suppl. 1991;9:S51–S55. - PubMed
-
- Barron AJ, Hughes AD, Sharp A, Baksi AJ, Surendran P, Jabbour RJ, Stanton A, Poulter N, Fitzgerald D, Sever P, O’Brien E, Thom S, Mayet J. Long-term antihypertensive treatment fails to improve E/e’ despite regression of left ventricular mass: an Anglo-Scandinavian cardiac outcomes trial substudy. Hypertension. 2014;63:252–258. - PubMed
-
- Bernardo BC, Weeks KL, Pretorius L, McMullen JR. Molecular distinction between physiological and pathological cardiac hypertrophy: experimental findings and therapeutic strategies. Pharmacol Ther. 2010;128:191–227. - PubMed
-
- Betocchi S, Chiariello M. Effects of antihypertensive therapy on diastolic dysfunction in left ventricular hypertrophy. J Cardiovasc Pharmacol. 1992;19(Suppl 5):S116–S121. - PubMed
-
- Bisping E, Wakula P, Poteser M, Heinzel FR. Targeting cardiac hypertrophy: toward a causal heart failure therapy. J Cardiovasc Pharmacol. 2014;64:293–305. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous