

A Pneumococcal Protein Array as a Platform to Discover Serodiagnostic Antigens Against Infection
- PMID: 26183717
- PMCID: PMC4597139
- DOI: 10.1074/mcp.M115.049544
A Pneumococcal Protein Array as a Platform to Discover Serodiagnostic Antigens Against Infection
Abstract
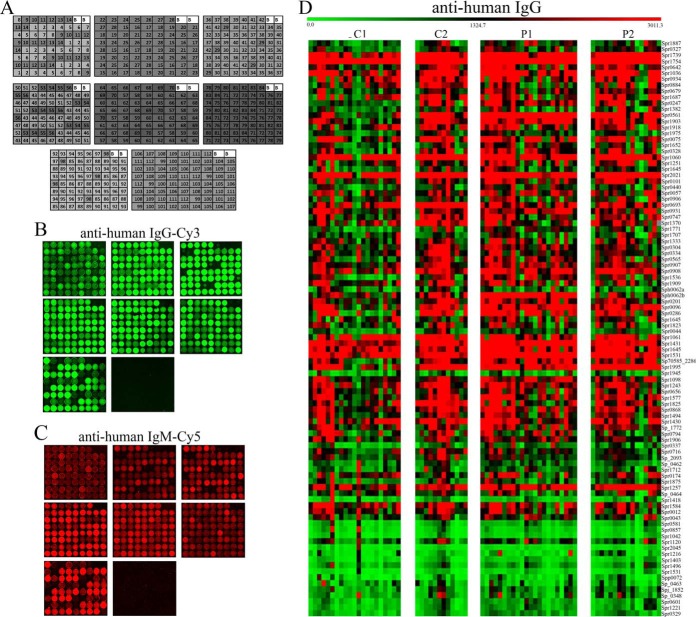
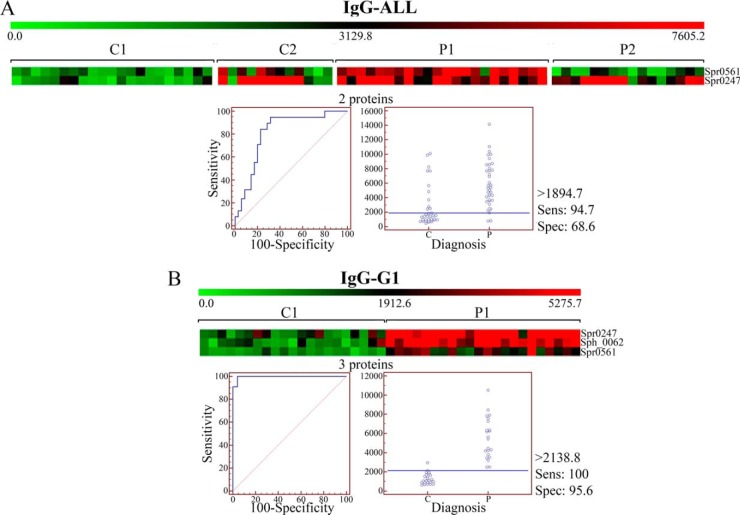
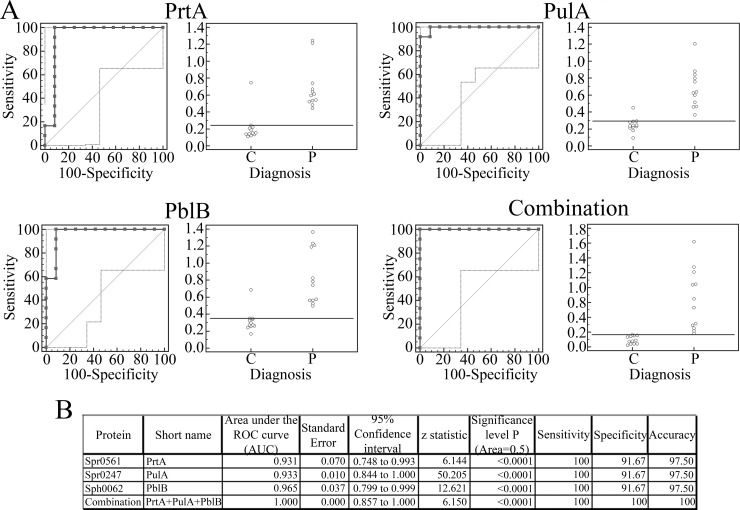
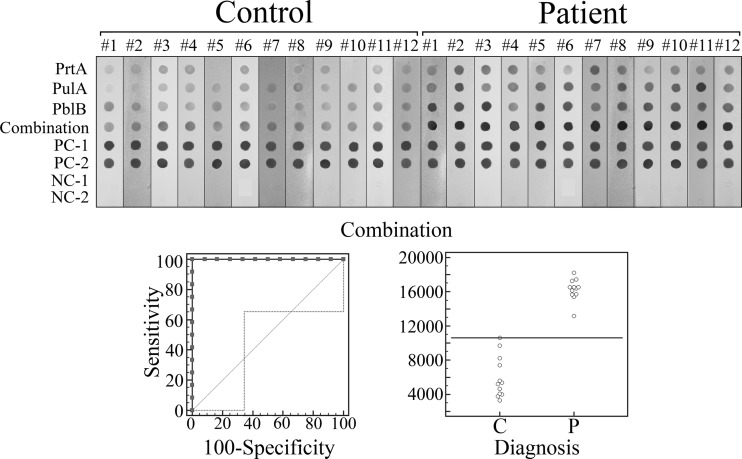
Pneumonia is one of the most common and severe diseases associated with Streptococcus pneumoniae infections in children and adults. Etiological diagnosis of pneumococcal pneumonia in children is generally challenging because of limitations of diagnostic tests and interference with nasopharyngeal colonizing strains. Serological assays have recently gained interest to overcome some problems found with current diagnostic tests in pediatric pneumococcal pneumonia. To provide insight into this field, we have developed a protein array to screen the antibody response to many antigens simultaneously. Proteins were selected by experimental identification from a collection of 24 highly prevalent pediatric clinical isolates in Spain, using a proteomics approach consisting of "shaving" the cell surface with proteases and further LC/MS/MS analysis. Ninety-five proteins were recombinantly produced and printed on an array. We probed it with a collection of sera from children with pneumococcal pneumonia. From the set of the most seroprevalent antigens, we obtained a clear discriminant response for a group of three proteins (PblB, PulA, and PrtA) in children under 4 years old. We validated the results by ELISA and an immunostrip assay showed the translation to easy-to-use, affordable tests. Thus, the protein array here developed presents a tool for broad use in serodiagnostics.
© 2015 by The American Society for Biochemistry and Molecular Biology, Inc.
Figures

Similar articles
-
Synchrony in serum antibody response to conserved proteins of Streptococcus pneumoniae in young children.Hum Vaccin Immunother. 2015;11(2):489-97. doi: 10.4161/21645515.2014.990861. Hum Vaccin Immunother. 2015. PMID: 25692218 Free PMC article.
-
Failure to elicit seroresponses to pneumococcal surface proteins (pneumococcal histidine triad D, pneumococcal choline-binding protein A, and serine proteinase precursor A) in children with pneumococcal bacteraemia.Clin Microbiol Infect. 2012 Aug;18(8):756-62. doi: 10.1111/j.1469-0691.2011.03629.x. Epub 2011 Aug 18. Clin Microbiol Infect. 2012. PMID: 21851490
-
Assessment of an Antibody-in-Lymphocyte Supernatant Assay for the Etiological Diagnosis of Pneumococcal Pneumonia in Children.Front Cell Infect Microbiol. 2020 Jan 17;9:459. doi: 10.3389/fcimb.2019.00459. eCollection 2019. Front Cell Infect Microbiol. 2020. PMID: 32039044 Free PMC article.
-
Proteomics-driven design of a multiplex bead-based platform to assess natural IgG antibodies to pneumococcal protein antigens in children.J Proteomics. 2015 Aug 3;126:228-33. doi: 10.1016/j.jprot.2015.06.011. Epub 2015 Jun 26. J Proteomics. 2015. PMID: 26122914
-
Current status and perspectives on protein-based pneumococcal vaccines.Crit Rev Microbiol. 2015 Jun;41(2):190-200. doi: 10.3109/1040841X.2013.813902. Epub 2013 Jul 29. Crit Rev Microbiol. 2015. PMID: 23895377 Review.
Cited by
-
Prediction and Validation of Immunogenic Domains of Pneumococcal Proteins Recognized by Human CD4+ T Cells.Infect Immun. 2019 May 21;87(6):e00098-19. doi: 10.1128/IAI.00098-19. Print 2019 Jun. Infect Immun. 2019. PMID: 30910792 Free PMC article.
-
Approaching In Vivo Models of Pneumococcus-Host Interaction: Insights into Surface Proteins, Capsule Production, and Extracellular Vesicles.Pathogens. 2021 Aug 28;10(9):1098. doi: 10.3390/pathogens10091098. Pathogens. 2021. PMID: 34578131 Free PMC article.
-
Data in support of proteomic analysis of pneumococcal pediatric clinical isolates to construct a protein array.Data Brief. 2016 Feb 5;6:917-22. doi: 10.1016/j.dib.2016.01.057. eCollection 2016 Mar. Data Brief. 2016. PMID: 26949725 Free PMC article.
-
Diagnosis of Streptococcus pneumoniae infection using circulating antibody secreting cells.PLoS One. 2021 Nov 12;16(11):e0259644. doi: 10.1371/journal.pone.0259644. eCollection 2021. PLoS One. 2021. PMID: 34767590 Free PMC article.
-
Integrated proteomic and metabolomic analysis reveals that rhodomyrtone reduces the capsule in Streptococcus pneumoniae.Sci Rep. 2017 Jun 2;7(1):2715. doi: 10.1038/s41598-017-02996-3. Sci Rep. 2017. PMID: 28578394 Free PMC article.
References
-
- Vernet G., Saha S., Satzke C., Burgess D. H., Alderson M., Maisonneuve J. F., Beall B. W., Steinhoff M. C., Klugman K. P. (2011) Laboratory-based diagnosis of pneumococcal pneumonia: state of the art and unmet needs. Clin. Microbiol. Infect. 17, 1–13 - PubMed
-
- Johnson H. L., Deloria-Knoll M., Levine O. S., Stoszek S. K., Freimanis Hance L., Reithinger R., Muenz L. R., O'Brien K. L. (2010) Systematic evaluation of serotypes causing invasive pneumococcal disease among children under five: the pneumococcal global serotype project. PLoS Med. 7, e1000348. - PMC - PubMed
-
- Pittet L. F., Posfay-Barbe K. M. (2012) Pneumococcal vaccines for children: a global public health priority. Clin. Microbiol. Infect. 18, 25–36 - PubMed
-
- Welte T., Torres A., Nathwani D. (2012) Clinical and economic burden of community-acquired pneumonia among adults in Europe. Thorax 67, 71–79 - PubMed
-
- Weycker D., Strutton D., Edelsberg J., Sato R., Jackson L. A. (2010) Clinical and economic burden of pneumococcal disease in older US adults. Vaccine 28, 4955–4960 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
