

Cortisol-dependent stress effects on cell distribution in healthy individuals and individuals suffering from chronic adrenal insufficiency
- PMID: 26184081
- PMCID: PMC5526346
- DOI: 10.1016/j.bbi.2015.07.010
Cortisol-dependent stress effects on cell distribution in healthy individuals and individuals suffering from chronic adrenal insufficiency
Abstract
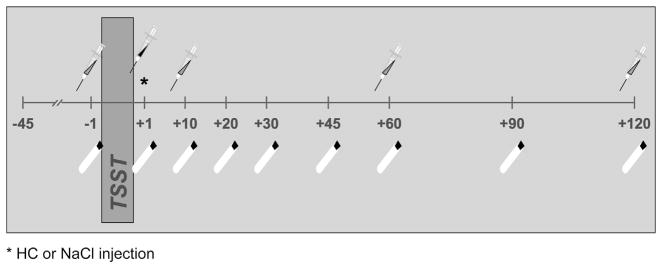
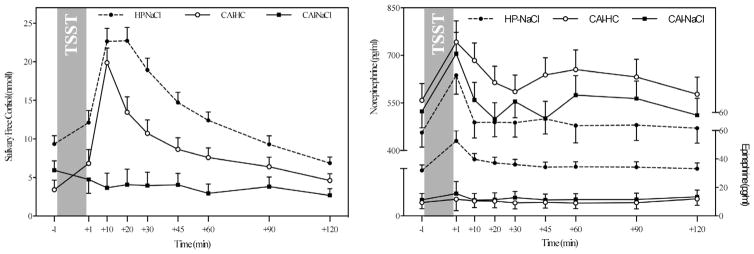
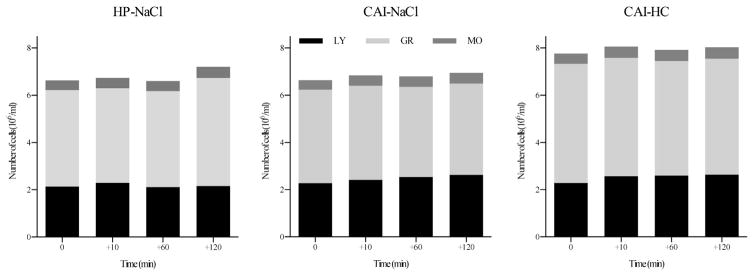
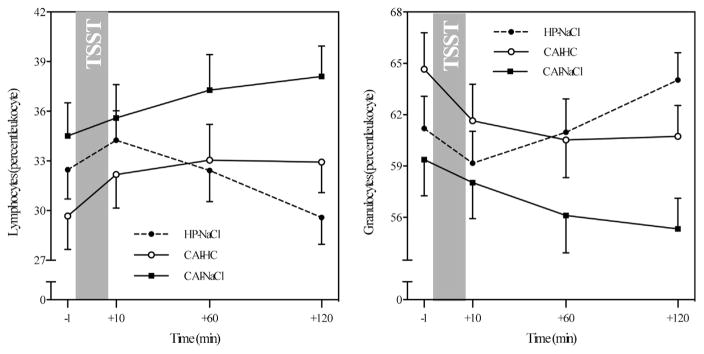
Chronic adrenal insufficiency (CAI) is characterized by a lack of glucocorticoid and mineralocorticoid production due to destroyed adrenal cortex cells. However, elevated cortisol secretion is thought to be a central part in a well-orchestrated immune response to stress. This raises the question to what extent lack of cortisol in CAI affects stress-related changes in immune processes. To address this question, 28 CAI patients (20 females) and 18 healthy individuals (11 females) (age: 44.3 ± 8.4 years) were exposed to a psychosocial stress test (Trier Social Stress Test: TSST). Half the patients received a 0.03 mg/kg body weight injection of hydrocortisone (HC) post-TSST to mimic a healthy cortisol stress response. Catecholamines and immune cell composition were assessed in peripheral blood and free cortisol measured in saliva collected before and repeatedly after TSST. CAI patients showed norepinephrine (NE) stress responses similar to healthy participants, however, epinephrine (E) as well as cortisol levels were significantly lower. HC treatment post-TSST resulted in cortisol increases comparable to those observed in healthy participants (interaction effects--NE: F=1.05, p=.41; E: F=2.56, p=.045; cortisol: F=13.28, p<.001). Healthy individuals showed the expected pattern of stress-related early lymphocyte increase with subsequent decrease below baseline. The opposite pattern was observed in granulocytes. While exhibiting a similar initial increase, lymphocytes kept increasing over the following 2h in untreated patients. HC treatment buffered this effect (interaction effects--lymphocyte%: F=7.31, p<.001; granulocyte%: F=7.71, p<.001). Using CAI in humans as a model confirms cortisol's central involvement in post-stress lymphocyte migration from blood into immune-relevant body compartments. As such, future studies should investigate whether psychosocial stress exposure may put CAI patients at an increased health risk due to attenuated immune responses to pathogens.
Keywords: Catecholamines; Cell trafficking; Chronic adrenal insufficiency; Cortisol; Psychosocial stress.
Copyright © 2015. Published by Elsevier Inc.
Conflict of interest statement
The authors declare no conflict of interests.
Figures
Similar articles
-
Peripheral Blood Leukocyte Subpopulation Changes in Reaction to an Acute Psychosocial Stressor as Compared to an Active Placebo-Stressor in Healthy Young Males: Mediating Effects of Major Stress-Reactive Endocrine Parameters.Cells. 2024 Nov 22;13(23):1941. doi: 10.3390/cells13231941. Cells. 2024. PMID: 39682690 Free PMC article.
-
Acute psychosocial stress induces differential short-term changes in catecholamine sensitivity of stimulated inflammatory cytokine production.Brain Behav Immun. 2015 Jan;43:139-48. doi: 10.1016/j.bbi.2014.07.014. Epub 2014 Aug 6. Brain Behav Immun. 2015. PMID: 25107875
-
Endocrine stress responses in TH1-mediated chronic inflammatory skin disease (psoriasis vulgaris)--do they parallel stress-induced endocrine changes in TH2-mediated inflammatory dermatoses (atopic dermatitis)?Psychoneuroendocrinology. 2006 May;31(4):439-46. doi: 10.1016/j.psyneuen.2005.10.006. Epub 2005 Dec 13. Psychoneuroendocrinology. 2006. PMID: 16359823 Clinical Trial.
-
Central adrenal insufficiency: who, when, and how? From the evidence to the controversies - an exploratory review.Arch Endocrinol Metab. 2022 Sept 08;66(4):541-550. doi: 10.20945/2359-3997000000493. Epub 2022 Jun 23. Arch Endocrinol Metab. 2022. PMID: 35758836 Free PMC article. Review.
-
Cultures under stress: A cross-national meta-analysis of cortisol responses to the Trier Social Stress Test and their association with anxiety-related value orientations and internalizing mental disorders.Psychoneuroendocrinology. 2019 Jul;105:147-154. doi: 10.1016/j.psyneuen.2018.12.236. Epub 2018 Dec 24. Psychoneuroendocrinology. 2019. PMID: 30611610 Review.
Cited by
-
Immune cell dynamics in response to an acute laboratory stressor: a within-person between-group analysis of the biological impact of early life adversity.Stress. 2022 Jan;25(1):347-356. doi: 10.1080/10253890.2022.2148100. Stress. 2022. PMID: 36404775 Free PMC article.
-
Essential oil from the roots of Paeonia lactiflora pall. has protective effect against corticosterone-induced depression in mice via modulation of PI3K/Akt signaling pathway.Front Pharmacol. 2022 Sep 16;13:999712. doi: 10.3389/fphar.2022.999712. eCollection 2022. Front Pharmacol. 2022. PMID: 36188568 Free PMC article.
-
Adrenal insufficiency.Nat Rev Dis Primers. 2021 Mar 11;7(1):19. doi: 10.1038/s41572-021-00252-7. Nat Rev Dis Primers. 2021. PMID: 33707469 Review.
-
Combined Effect Of Coffee Consumption And Cigarette Smoking On Serum Levels Of Vitamin B12, Folic Acid, And Lipid Profile In Young Male: A Cross-Sectional Study.Int J Gen Med. 2019 Nov 22;12:421-432. doi: 10.2147/IJGM.S213737. eCollection 2019. Int J Gen Med. 2019. PMID: 31819593 Free PMC article.
-
Peripheral Blood Leukocyte Subpopulation Changes in Reaction to an Acute Psychosocial Stressor as Compared to an Active Placebo-Stressor in Healthy Young Males: Mediating Effects of Major Stress-Reactive Endocrine Parameters.Cells. 2024 Nov 22;13(23):1941. doi: 10.3390/cells13231941. Cells. 2024. PMID: 39682690 Free PMC article.
References
-
- al-Shoumer KA, Beshyah SA, Niththyananthan R, Johnston DG. Effect of glucocorticoid replacement therapy on glucose tolerance and intermediary metabolites in hypopituitary adults. Clin Endocrinol (Oxf) 1995;42(1):85–90. - PubMed
-
- Arlt W, Allolio B. Adrenal insufficiency. Lancet. 2003;361(9372):1881–1893. - PubMed
-
- Benschop RJ, Rodriguez-Feuerhahn M, Schedlowski M. Catecholamine-induced leukocytosis: early observations, current research, and future directions. Brain Behav Immun. 1996;10(2):77–91. - PubMed
-
- Betterle C, Dal Pra C, Mantero F, Zanchetta R. Autoimmune adrenal insufficiency and autoimmune polyendocrine syndromes: autoantibodies, autoantigens, and their applicability in diagnosis and disease prediction. Endocr Rev. 2002;23(3):327–364. - PubMed
-
- Bornstein SR, Breidert M, Ehrhart-Bornstein M, Kloos B, Scherbaum WA. Plasma catecholamines in patients with Addison’s disease. Clin Endocrinol (Oxf) 1995;42(2):215–218. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
