

Combination Therapy Reverses Hyperglycemia in NOD Mice With Established Type 1 Diabetes
- PMID: 26185279
- PMCID: PMC4613966
- DOI: 10.2337/db15-0164
Combination Therapy Reverses Hyperglycemia in NOD Mice With Established Type 1 Diabetes
Abstract
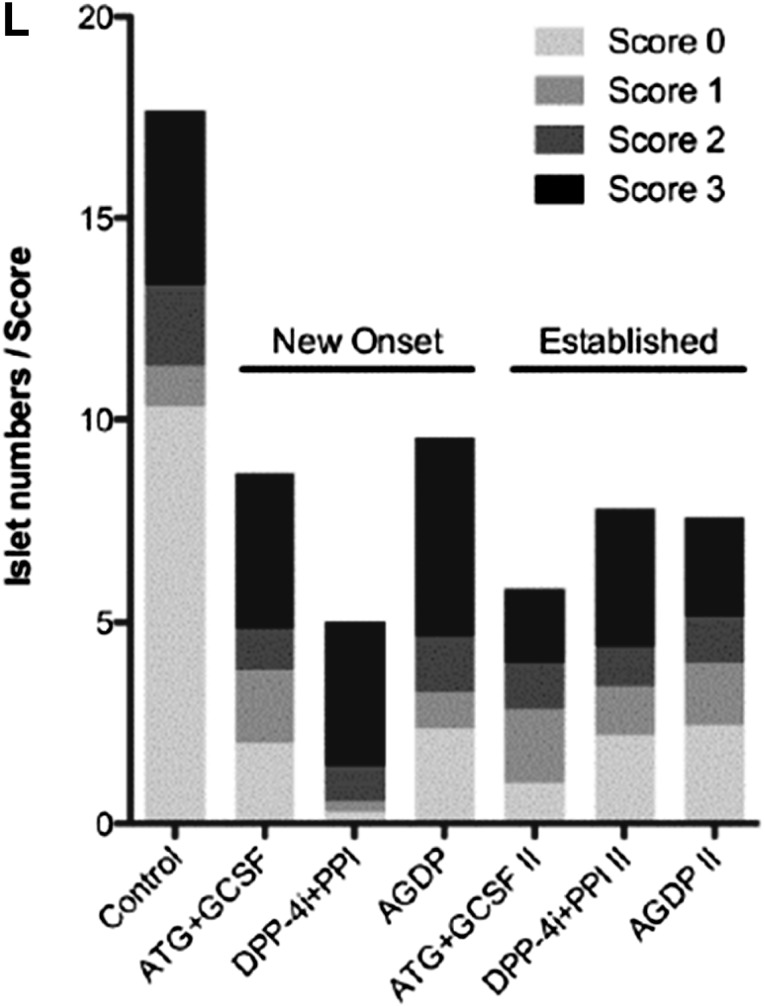
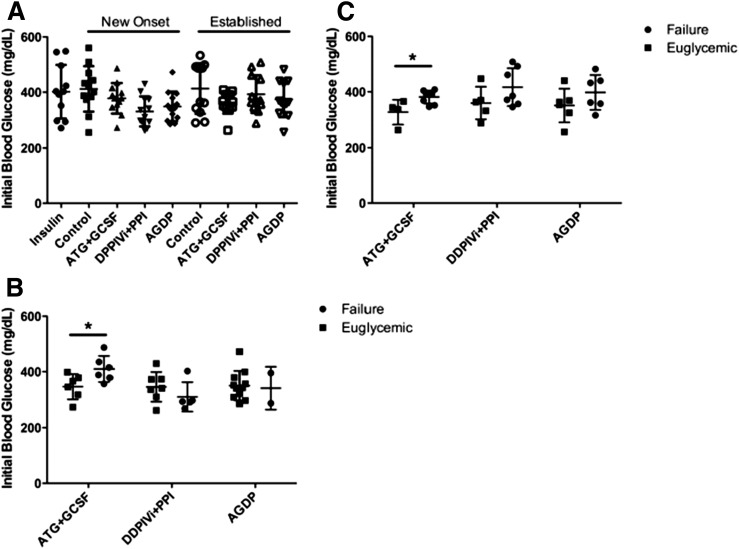
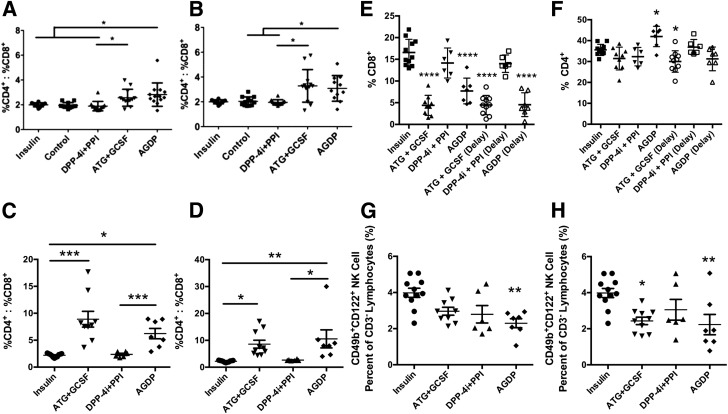
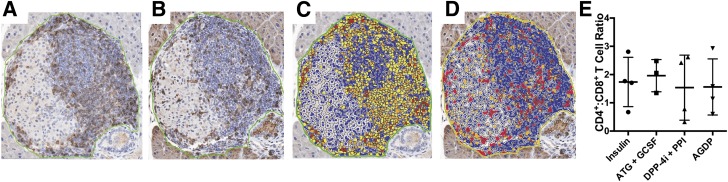
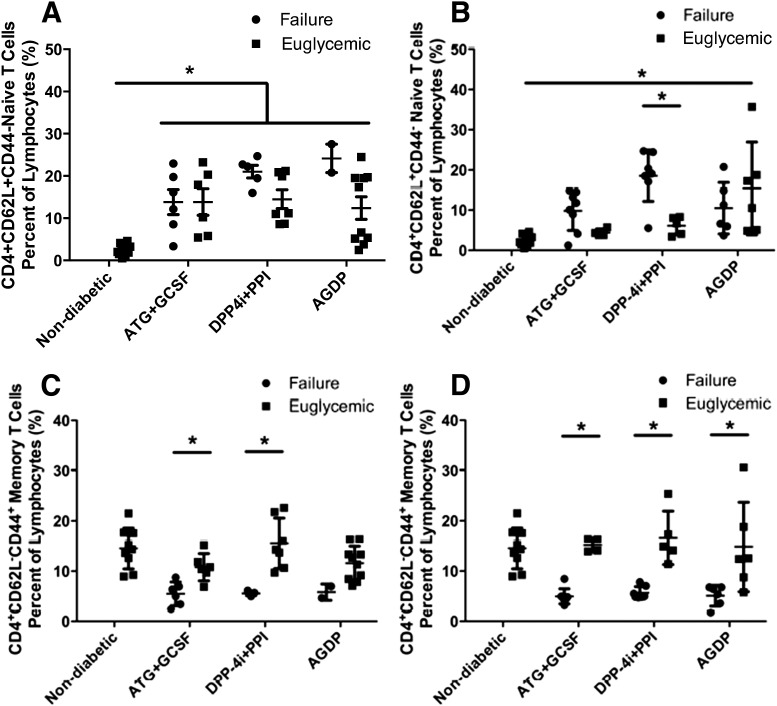
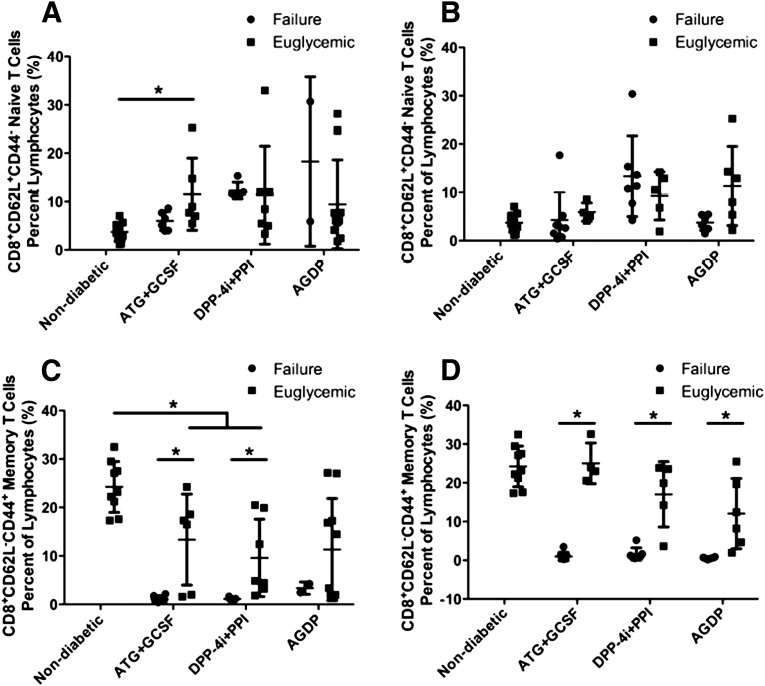
An increasing number of therapies have proven effective at reversing hyperglycemia in the nonobese diabetic (NOD) mouse model of type 1 diabetes (T1D), yet situations of successful translation to human T1D are limited. This may be partly due to evaluating the effect of treating immediately at diagnosis in mice, which may not be reflective of the advanced disease state in humans at disease onset. In this study, we treated NOD mice with new-onset as well as established disease using various combinations of four drugs: antithymocyte globulin (ATG), granulocyte-colony stimulating factor (G-CSF), a dipeptidyl peptidase IV inhibitor (DPP-4i), and a proton pump inhibitor (PPI). Therapy with all four drugs induced remission in 83% of new-onset mice and, remarkably, in 50% of NOD mice with established disease. Also noteworthy, disease remission occurred irrespective of initial blood glucose values and mechanistically was characterized by enhanced immunoregulation involving alterations in CD4+ T cells, CD8+ T cells, and natural killer cells. This combination therapy also allowed for effective treatment at reduced drug doses (compared with effective monotherapy), thereby minimizing potential adverse effects while retaining efficacy. This combination of approved drugs demonstrates a novel ability to reverse T1D, thereby warranting translational consideration.
© 2015 by the American Diabetes Association. Readers may use this article as long as the work is properly cited, the use is educational and not for profit, and the work is not altered.
Figures



References
-
- Atkinson MA, Eisenbarth GS. Type 1 diabetes: new perspectives on disease pathogenesis and treatment. Lancet 2001;358:221–229 - PubMed
-
- Anderson MS, Bluestone JA. The NOD mouse: a model of immune dysregulation. Annu Rev Immunol 2005;23:447–485 - PubMed
-
- Atkinson MA. Evaluating preclinical efficacy. Sci Transl Med 2011;3:96cm22. - PubMed
-
- Herold KC, Bluestone JA. Type 1 diabetes immunotherapy: is the glass half empty or half full? Sci Transl Med 2011;3:95fs1. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
