

The Efficacy of Gabapentin in Patients with Central Post-stroke Pain
- PMID: 26185510
- PMCID: PMC4499431
The Efficacy of Gabapentin in Patients with Central Post-stroke Pain
Abstract
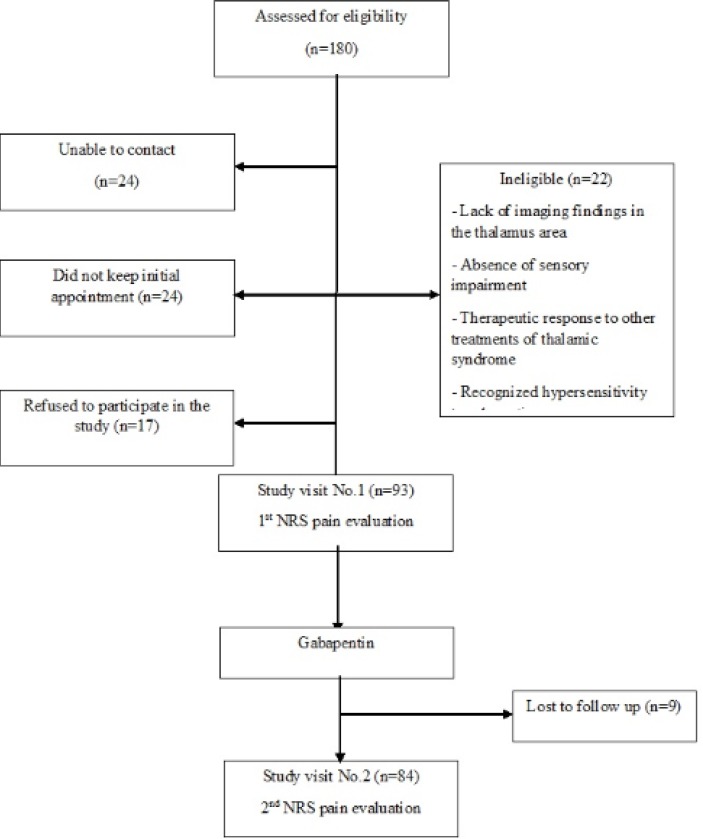
Thalamic pain syndrome, a type of central post-stroke pain (CPSP), may develops after a hemorrhagic or ischemic stroke and results in impairment of the thalamus. There is limited experience about gabapentin in treatment of central pains like CPSP. In a prospective observational study, the intensity of pain was recorded using the Numeric Rating Scale (NRS) at the entrance to the study. Patients eligible for treating with gabapentin, received gabapentin 300 mg twice-daily. The pain intensity was measured at entrance to the study and after one month using NRS. Decrease of 3 points from the initial NRS considered being clinically significant. From a total of 180 primarily screened patients, 84 (44 men and 40 women) were recruited. There was a significant difference between pre-treatment and post-treatment NRS (5.9 ± 2.51 vs. 4.7 ± 3.01; 95% CI: 0.442-1.962, p = 0.002). Fisher's exact test showed no statistically significant effect of clinical and demographic characteristics of patients on their therapeutic response to gabapentin. Given the safety, efficacy, well tolerability and lack of interaction with other drugs we suggest gabapentin to be more considered as a first line therapy or as add-on therapy for reducing the pain severity in patients with thalamic syndrome.
Keywords: Central nervous system; Central post stroke pain; Cerebrovascular accident; Gabapentin.
Figures
References
-
- Klit H, Finnerup NB, Jensen TS. Central post-stroke pain: clinical characteristics, pathophysiology, and management. Lancet Neurol. 2009;8:857–868. - PubMed
-
- Klit H, Finnerup NB, Andersen G, Jensen TS. Central poststroke pain: a population-based study. Pain. 2011;152:818–824. - PubMed
-
- Cepeda MS, Africano JM, Polo R, Alcala R, Carr DB. What decline in pain intensity is meaningful to patients with acute pain? Pain. 2003;105:151–157. - PubMed
-
- Kumar B, Kalita J, Kumar G, Misra UK. Central poststroke pain: a review of pathophysiology and treatment. Anesth. Analg. 2009;108:1645–1657. - PubMed
-
- Harvey RL. Central poststroke pain syndrome. Top Stroke Rehabil. 2010;17:163–172. - PubMed
LinkOut - more resources
Full Text Sources