

The System-Wide Effect of Real-Time Audiovisual Feedback and Postevent Debriefing for In-Hospital Cardiac Arrest: The Cardiopulmonary Resuscitation Quality Improvement Initiative
- PMID: 26186567
- PMCID: PMC4603366
- DOI: 10.1097/CCM.0000000000001202
The System-Wide Effect of Real-Time Audiovisual Feedback and Postevent Debriefing for In-Hospital Cardiac Arrest: The Cardiopulmonary Resuscitation Quality Improvement Initiative
Abstract
Objective: To evaluate the effect of implementing real-time audiovisual feedback with and without postevent debriefing on survival and quality of cardiopulmonary resuscitation quality at in-hospital cardiac arrest.
Design: A two-phase, multicentre prospective cohort study.
Setting: Three UK hospitals, all part of one National Health Service Acute Trust.
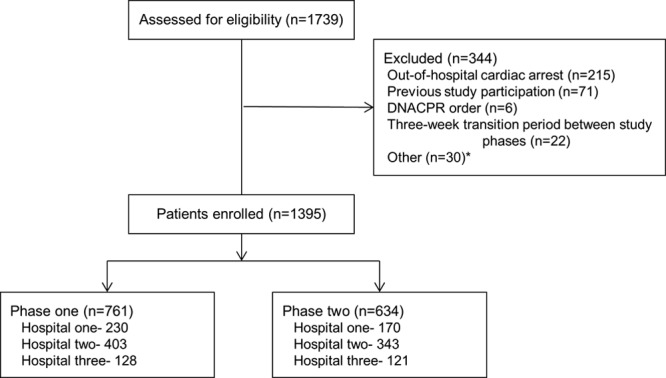
Patients: One thousand three hundred and ninety-five adult patients who sustained an in-hospital cardiac arrest at the study hospitals and were treated by hospital emergency teams between November 2009 and May 2013.
Interventions: During phase 1, quality of cardiopulmonary resuscitation and patient outcomes were measured with no intervention implemented. During phase 2, staff at hospital 1 received real-time audiovisual feedback, whereas staff at hospital 2 received real-time audiovisual feedback supplemented by postevent debriefing. No intervention was implemented at hospital 3 during phase 2.
Measurements and main results: The primary outcome was return of spontaneous circulation. Secondary endpoints included other patient-focused outcomes, such as survival to hospital discharge, and process-focused outcomes, such as chest compression depth. Random-effect logistic and linear regression models, adjusted for baseline patient characteristics, were used to analyze the effect of the interventions on study outcomes. In comparison with no intervention, neither real-time audiovisual feedback (adjusted odds ratio, 0.62; 95% CI, 0.31-1.22; p=0.17) nor real-time audiovisual feedback supplemented by postevent debriefing (adjusted odds ratio, 0.65; 95% CI, 0.35-1.21; p=0.17) was associated with a statistically significant improvement in return of spontaneous circulation or any process-focused outcome. Despite this, there was evidence of a system-wide improvement in phase 2, leading to improvements in return of spontaneous circulation (adjusted odds ratio, 1.87; 95% CI, 1.06-3.30; p=0.03) and process-focused outcomes.
Conclusions: Implementation of real-time audiovisual feedback with or without postevent debriefing did not lead to a measured improvement in patient or process-focused outcomes at individual hospital sites. However, there was an unexplained system-wide improvement in return of spontaneous circulation and process-focused outcomes during the second phase of the study.
Figures
Comment in
-
Quality Cardiopulmonary Resuscitation: Aspirational, But Not Enough?Crit Care Med. 2015 Nov;43(11):2508-9. doi: 10.1097/CCM.0000000000001237. Crit Care Med. 2015. PMID: 26468703 No abstract available.
References
-
- Vaillancourt C, Everson-Stewart S, Christenson J, et al. Resuscitation Outcomes Consortium Investigators. The impact of increased chest compression fraction on return of spontaneous circulation for out-of-hospital cardiac arrest patients not in ventricular fibrillation. Resuscitation. 2011;82:1501–1507. - PMC - PubMed
-
- Idris AH, Guffey D, Pepe PE, et al. Resuscitation Outcomes Consortium Investigators. Chest compression rates and survival following out-of-hospital cardiac arrest. Crit Care Med. 2015;43:840–848. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
