

Effectiveness of Case Management for 'At Risk' Patients in Primary Care: A Systematic Review and Meta-Analysis
- PMID: 26186598
- PMCID: PMC4505905
- DOI: 10.1371/journal.pone.0132340
Effectiveness of Case Management for 'At Risk' Patients in Primary Care: A Systematic Review and Meta-Analysis
Abstract
Background: An ageing population with multimorbidity is putting pressure on health systems. A popular method of managing this pressure is identification of patients in primary care 'at-risk' of hospitalisation, and delivering case management to improve outcomes and avoid admissions. However, the effectiveness of this model has not been subjected to rigorous quantitative synthesis.
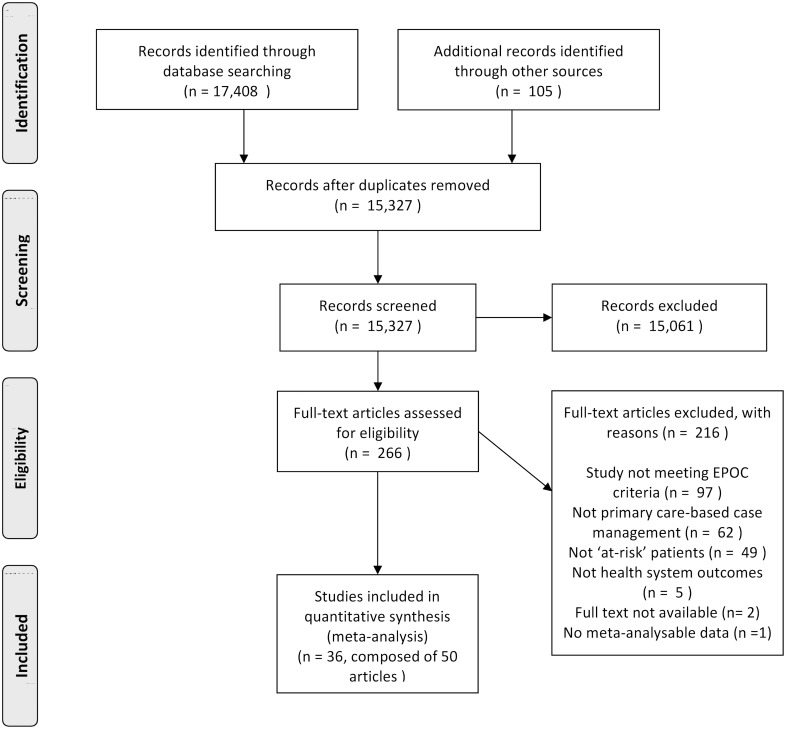
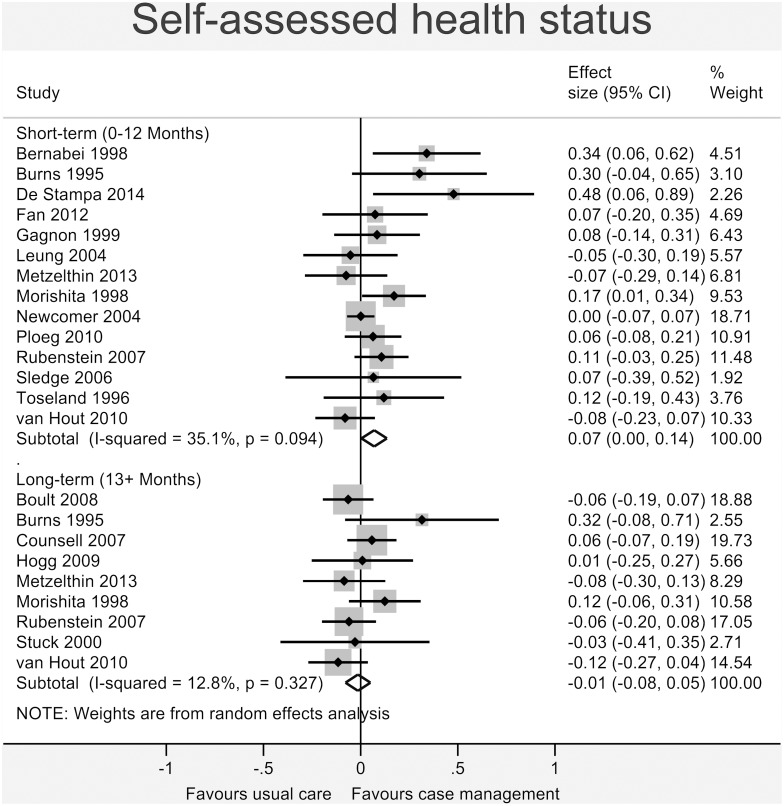
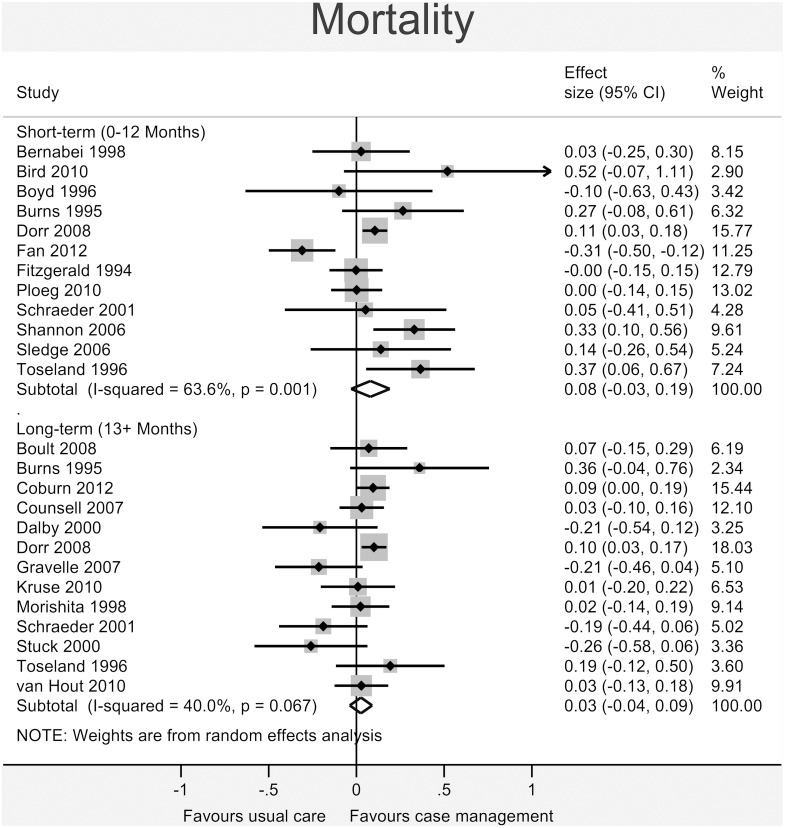
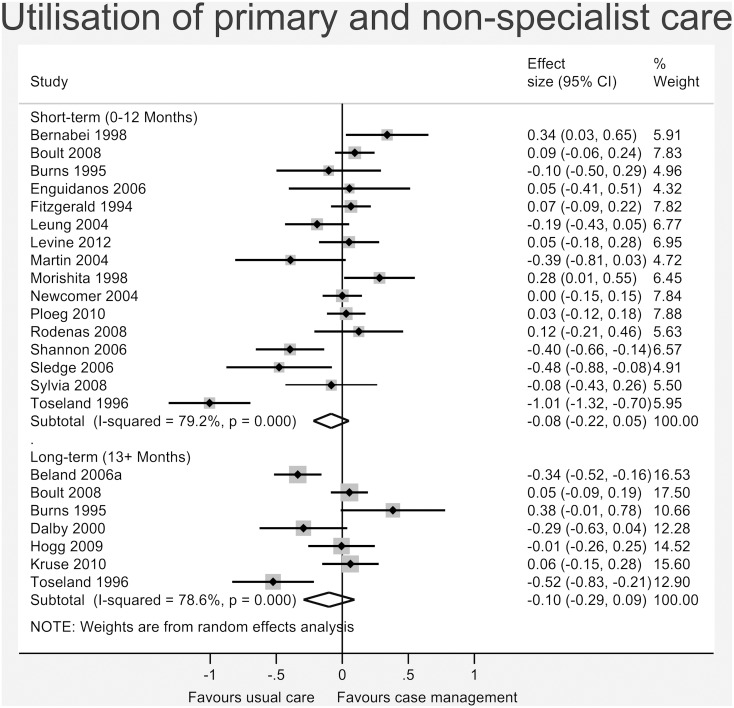
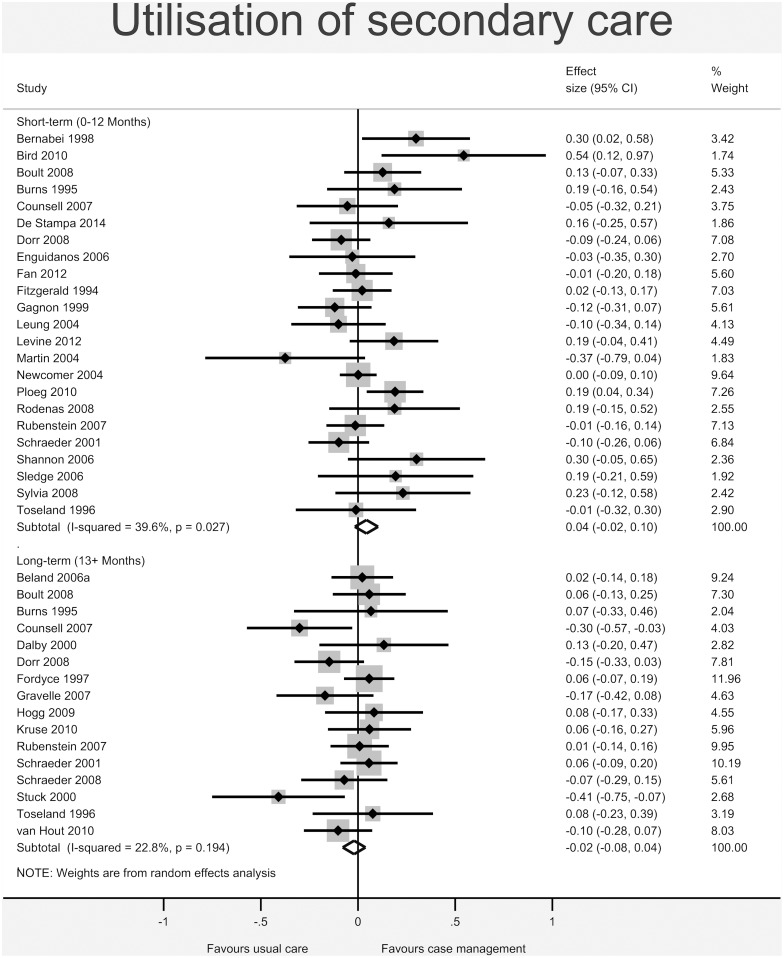
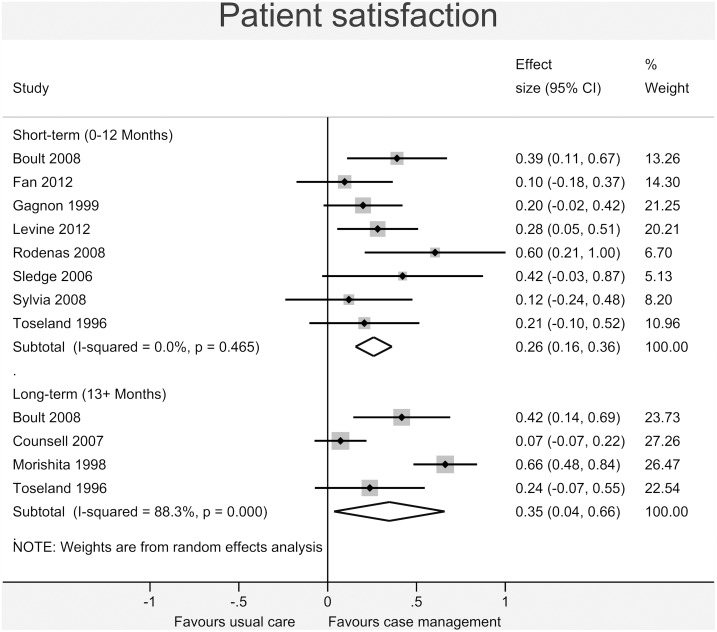
Methods and findings: We carried out a systematic review and meta-analysis of the effectiveness of case management for 'at-risk' patients in primary care. Six bibliographic databases were searched using terms for 'case management', 'primary care', and a methodology filter (Cochrane EPOC group). Effectiveness compared to usual care was measured across a number of relevant outcomes: Health--self-assessed health status, mortality; Cost--total cost of care, healthcare utilisation (primary and non-specialist care and secondary care separately), and; Satisfaction--patient satisfaction. We conducted secondary subgroup analyses to assess whether effectiveness was moderated by the particular model of case management, context, and study design. A total of 15,327 titles and abstracts were screened, 36 unique studies were included. Meta-analyses showed no significant differences in total cost, mortality, utilisation of primary or secondary care. A very small significant effect favouring case management was found for self-reported health status in the short-term (0.07, 95% CI 0.00 to 0.14). A small significant effect favouring case management was found for patient satisfaction in the short- (0.26, 0.16 to 0.36) and long-term (0.35, 0.04 to 0.66). Secondary subgroup analyses suggested the effectiveness of case management may be increased when delivered by a multidisciplinary team, when a social worker was involved, and when delivered in a setting rated as low in initial 'strength' of primary care.
Conclusions: This was the first meta-analytic review which examined the effects of case management on a wide range of outcomes and considered also the effects of key moderators. Current results do not support case management as an effective model, especially concerning reduction of secondary care use or total costs. We consider reasons for lack of effect and highlight key research questions for the future.
Review protocol: The review protocol is available as part of the PROSPERO database (registration number: CRD42014010824).
Conflict of interest statement
Figures

References
-
- Nolte E, McKee M. Caring for people with chronic conditions: a health system perspective: McGraw-Hill International; 2008.
-
- Ham C, Walsh N. Making integrated care happen at scale and pace. London: The King's Fund, 2013.
-
- Atun R, Aydin S, Chakraborty S, Sümer S, Aran M, Gürol I, et al. Universal health coverage in Turkey: enhancement of equity. The Lancet. 2013;382(9886):65–99. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
