

Balancing Long-Term Risks of Ischemic and Bleeding Complications After Percutaneous Coronary Intervention With Drug-Eluting Stents
- PMID: 26187674
- PMCID: PMC4670082
- DOI: 10.1016/j.amjcard.2015.05.036
Balancing Long-Term Risks of Ischemic and Bleeding Complications After Percutaneous Coronary Intervention With Drug-Eluting Stents
Abstract
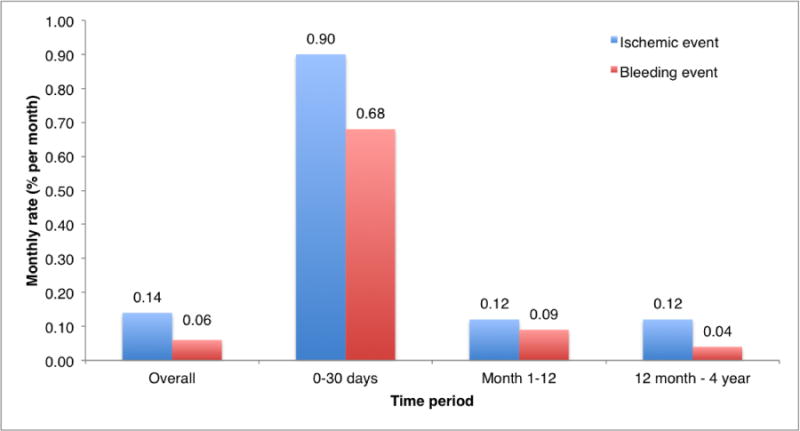
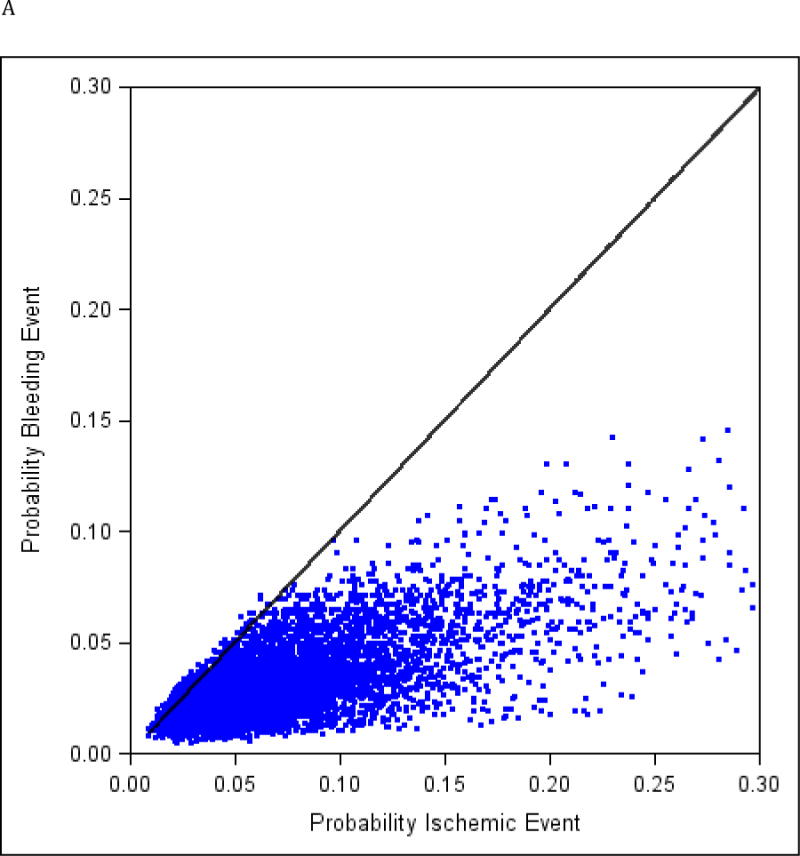
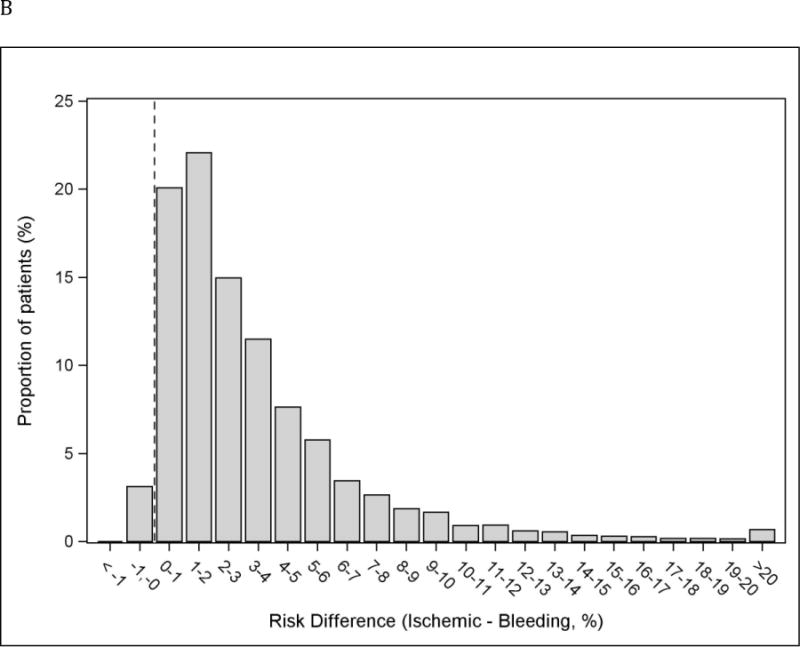
Although trials comparing antiplatelet strategies after percutaneous coronary intervention report average risks of bleeding and ischemia in a population, there is limited information to guide choices based on individual patient risks, particularly beyond 1 year after treatment. Patient-level data from Patient Related Outcomes With Endeavor vs Cypher Stenting Trial (PROTECT), a broadly inclusive trial enrolling 8,709 subjects treated with drug-eluting stents (sirolimus vs zotarolimus-eluting stent), and PROTECT US, a single-arm study including 1,018 subjects treated with a zotarolimus-eluting stent, were combined. The risk of ischemic events, cardiovascular death/non-periprocedural myocardial infarction (MI)/definite or probable stent thrombosis, and bleeding events, Global Use of Strategies to Open Occluded Arteries moderate or severe bleed, were predicted using logistic regression. At median follow-up of 4.1 years, major bleeding occurred in 260 subjects (2.8%) and ischemic events in 595 (6.3%). Multivariate predictors of bleeding were older age, smoking, diabetes mellitus, congestive heart failure, and chronic kidney disease (all p <0.05). Ischemic events shared all the same predictors with bleeding events and gender, body mass index, previous MI, previous coronary artery bypass graft surgery, ST-segment elevation MI on presentation, stent length, and sirolimus-eluting stent use (all p <0.05). Within individual subjects, bleeding and ischemic risks were strongly correlated; 97% of subjects had a greater risk of ischemic events than bleeding. In conclusion, individual patient risks of ischemia and bleeding are related to many common risk factors, yet the predicted risks of ischemic events are greater than those of major bleeding in the large majority of patients in long-term follow-up.
Copyright © 2015 Elsevier Inc. All rights reserved.
Figures
References
-
- Eisenstein EL, Anstrom KJ, Kong DF, Shaw LK, Tuttle RH, Mark DB, Kramer JM, Harrington RA, Matchar DB, Kandzari DE, Peterson ED, Schulman KA, Califf RM. Clopidogrel use and long-term clinical outcomes after drug-eluting stent implantation. JAMA. 2007;297:159–68. - PubMed
-
- Levine GN, Bates ER, Blankenship JC, Bailey SR, Bittl JA, Cercek B, Chambers CE, Ellis SG, Guyton RA, Hollenberg SM, Khot UN, Lange RA, Mauri L, Mehran R, Moussa ID, Mukherjee D, Nallamothu BK, Ting HH. 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. Circulation. 2011;124:e574–651. - PubMed
-
- Task Force on Myocardial Revascularization of the European Society of C, the European Association for Cardio-Thoracic S, European Association for Percutaneous Cardiovascular I. Wijns W, Kolh P, Danchin N, Di Mario C, Falk V, Folliguet T, Garg S, Huber K, James S, Knuuti J, Lopez-Sendon J, Marco J, Menicanti L, Ostojic M, Piepoli MF, Pirlet C, Pomar JL, Reifart N, Ribichini FL, Schalij MJ, Sergeant P, Serruys PW, Silber S, Sousa Uva M, Taggart D. Guidelines on myocardial revascularization. Eur Heart J. 2010;31:2501–55. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
