

Effect of adding mFOLFOX6 after neoadjuvant chemoradiation in locally advanced rectal cancer: a multicentre, phase 2 trial
- PMID: 26187751
- PMCID: PMC4670237
- DOI: 10.1016/S1470-2045(15)00004-2
Effect of adding mFOLFOX6 after neoadjuvant chemoradiation in locally advanced rectal cancer: a multicentre, phase 2 trial
Abstract
Background: Patients with locally advanced rectal cancer who achieve a pathological complete response to neoadjuvant chemoradiation have an improved prognosis. The need for surgery in these patients has been questioned, but the proportion of patients achieving a pathological complete response is small. We aimed to assess whether adding cycles of mFOLFOX6 between chemoradiation and surgery increased the proportion of patients achieving a pathological complete response.
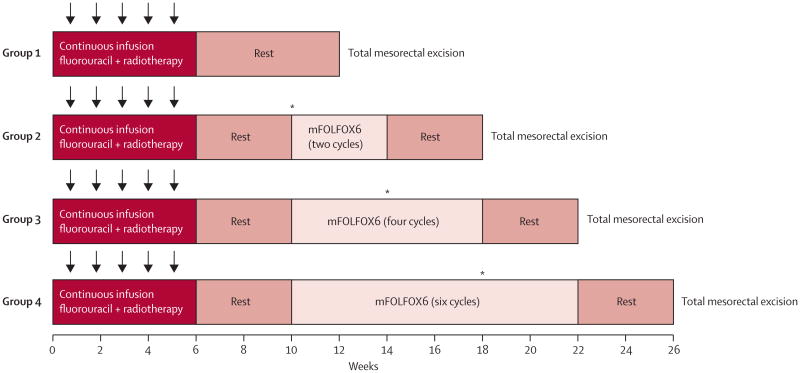
Methods: We did a phase 2, non-randomised trial consisting of four sequential study groups of patients with stage II-III locally advanced rectal cancer at 17 institutions in the USA and Canada. All patients received chemoradiation (fluorouracil 225 mg/m(2) per day by continuous infusion throughout radiotherapy, and 45·0 Gy in 25 fractions, 5 days per week for 5 weeks, followed by a minimum boost of 5·4 Gy). Patients in group 1 had total mesorectal excision 6-8 weeks after chemoradiation. Patients in groups 2-4 received two, four, or six cycles of mFOLFOX6, respectively, between chemoradiation and total mesorectal excision. Each cycle of mFOLFOX6 consisted of racemic leucovorin 200 mg/m(2) or 400 mg/m(2), according to the discretion of the treating investigator, oxaliplatin 85 mg/m(2) in a 2-h infusion, bolus fluorouracil 400 mg/m(2) on day 1, and a 46-h infusion of fluorouracil 2400 mg/m(2). The primary endpoint was the proportion of patients who achieved a pathological complete response, analysed by intention to treat. This trial is registered with ClinicalTrials.gov, number NCT00335816.
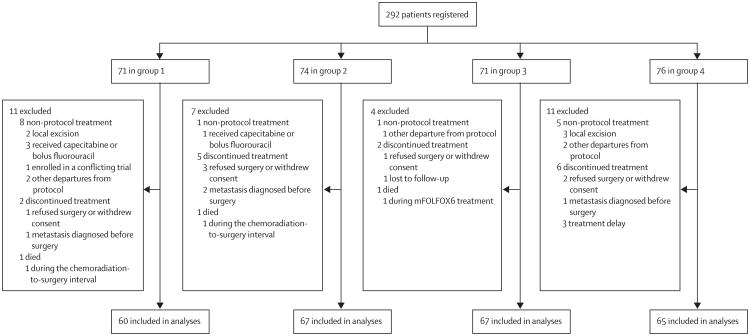
Findings: Between March 24, 2004, and Nov 16, 2012, 292 patients were registered, 259 of whom (60 in group 1, 67 in group 2, 67 in group 3, and 65 in group 4) met criteria for analysis. 11 (18%, 95% CI 10-30) of 60 patients in group 1, 17 (25%, 16-37) of 67 in group 2, 20 (30%, 19-42) of 67 in group 3, and 25 (38%, 27-51) of 65 in group 4 achieved a pathological complete response (p=0·0036). Study group was independently associated with pathological complete response (group 4 compared with group 1 odds ratio 3·49, 95% CI 1·39-8·75; p=0·011). In group 2, two (3%) of 67 patients had grade 3 adverse events associated with the neoadjuvant administration of mFOLFOX6 and one (1%) had a grade 4 adverse event; in group 3, 12 (18%) of 67 patients had grade 3 adverse events; in group 4, 18 (28%) of 65 patients had grade 3 adverse events and five (8%) had grade 4 adverse events. The most common grade 3 or higher adverse events associated with the neoadjuvant administration of mFOLFOX6 across groups 2-4 were neutropenia (five in group 3 and six in group 4) and lymphopenia (three in group 3 and four in group 4). Across all study groups, 25 grade 3 or worse surgery-related complications occurred (ten in group 1, five in group 2, three in group 3, and seven in group 4); the most common were pelvic abscesses (seven patients) and anastomotic leaks (seven patients).
Interpretation: Delivery of mFOLFOX6 after chemoradiation and before total mesorectal excision has the potential to increase the proportion of patients eligible for less invasive treatment strategies; this strategy is being tested in phase 3 clinical trials.
Funding: National Institutes of Health National Cancer Institute.
Trial registration: ClinicalTrials.gov NCT00335816 NCT02008656.
Copyright © 2015 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Extending neoadjuvant chemotherapy in rectal cancer.Lancet Oncol. 2015 Aug;16(8):880-1. doi: 10.1016/S1470-2045(15)00092-3. Epub 2015 Jul 14. Lancet Oncol. 2015. PMID: 26187752 No abstract available.
-
Gastrointestinal Cancers-Changing the Standard for Rectal Cancer and Establishing a New Standard for Liver Tumors.Int J Radiat Oncol Biol Phys. 2016 Jul 1;95(3):930-6. doi: 10.1016/j.ijrobp.2016.02.024. Int J Radiat Oncol Biol Phys. 2016. PMID: 27302509 Free PMC article. No abstract available.
References
-
- Sauer R, Becker H, Hohenberger W, et al. Preoperative versus postoperative chemoradiotherapy for rectal cancer. N Engl J Med. 2004;351:1731–40. - PubMed
-
- Williams NS, Johnston D. The quality of life after rectal excision for low rectal cancer. Br J Surg. 1983;70:460–62. - PubMed
-
- Maas M, Nelemans PJ, Valentini V, et al. Long-term outcome in patients with a pathological complete response after chemoradiation for rectal cancer: a pooled analysis of individual patient data. Lancet Oncol. 2010;11:835–44. - PubMed
-
- Smith JD, Ruby JA, Goodman KA, et al. Nonoperative management of rectal cancer with complete clinical response after neoadjuvant therapy. Ann Surg. 2012;256:965–72. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
