

Impaired upper esophageal sphincter reflexes in patients with supraesophageal reflux disease
- PMID: 26188682
- PMCID: PMC4628603
- DOI: 10.1053/j.gastro.2015.07.007
Impaired upper esophageal sphincter reflexes in patients with supraesophageal reflux disease
Abstract
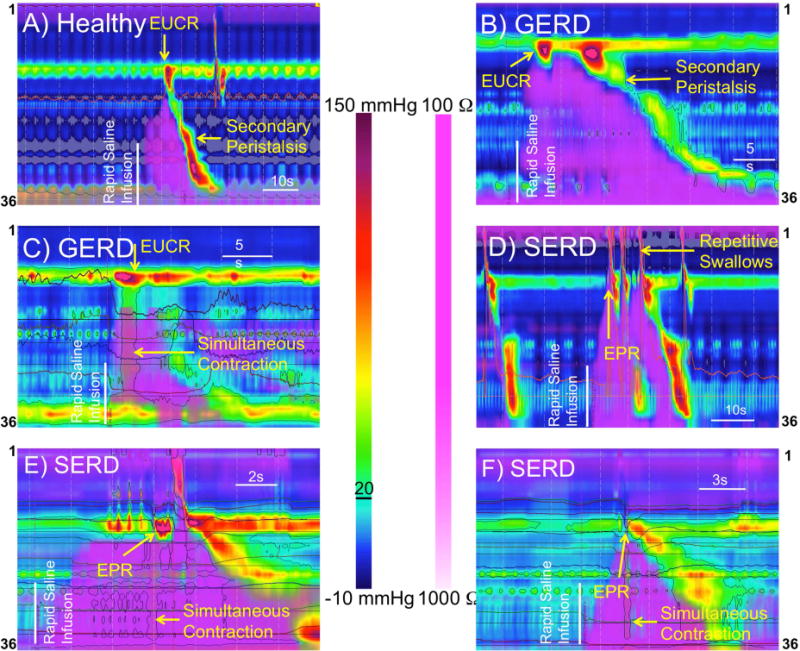
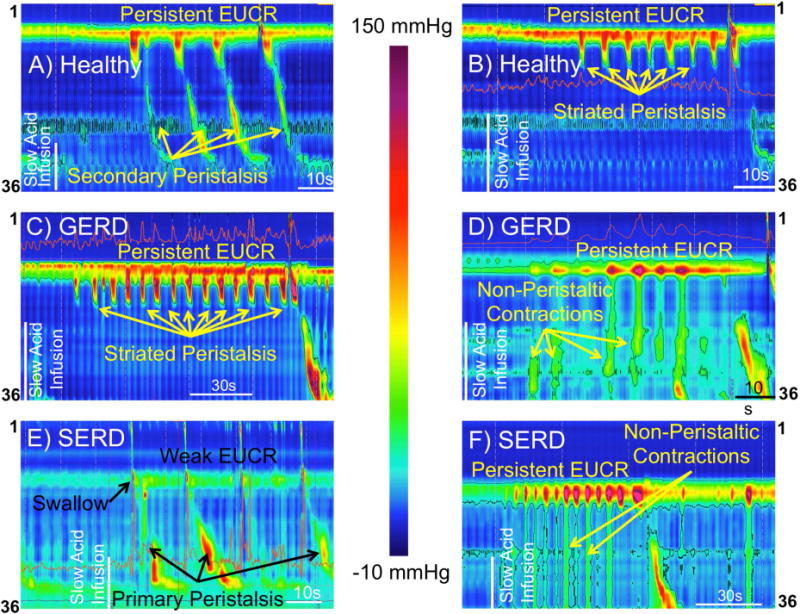
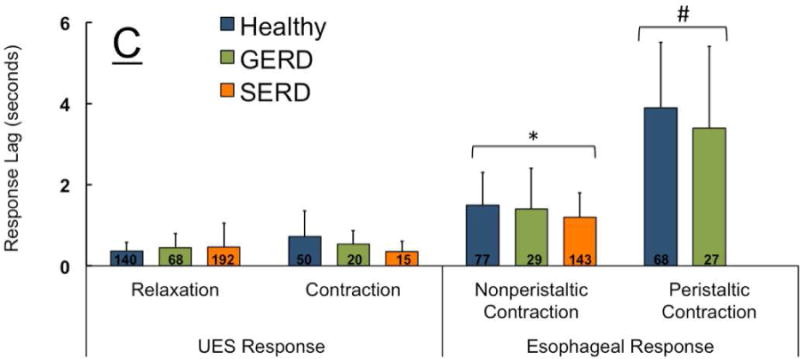
Background & aims: Normal responses of the upper esophageal sphincter (UES) and esophageal body to liquid reflux events prevent esophagopharyngeal reflux and its complications, however, abnormal responses have not been characterized. We investigated whether patients with supraesophageal reflux disease (SERD) have impaired UES and esophageal body responses to simulated reflux events.
Methods: We performed a prospective study of 25 patients with SERD (age, 19-82 y; 13 women) and complaints of regurgitation and supraesophageal manifestations of reflux. We also included 10 patients with gastroesophageal reflux disease (GERD; age, 32-60 y; 7 women) without troublesome regurgitation and supraesophageal symptoms and 24 healthy asymptomatic individuals (controls: age, 19-49 y; 13 women). UES and esophageal body pressure responses, along with luminal distribution of infusate during esophageal rapid and slow infusion of air or liquid, were monitored by concurrent high-resolution manometry and intraluminal impedance.
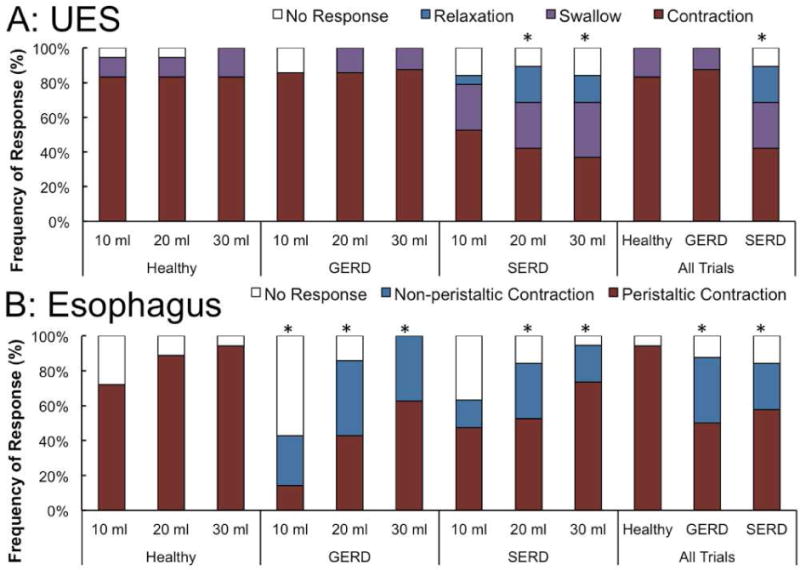
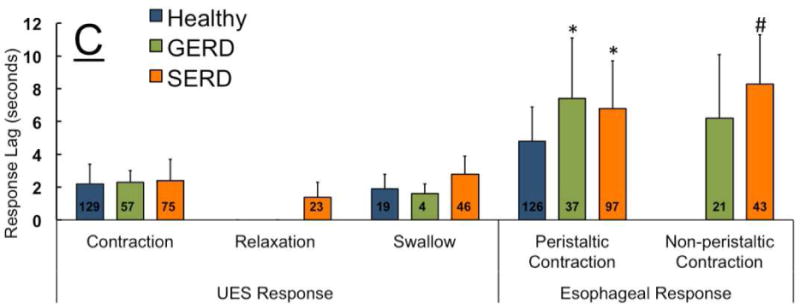
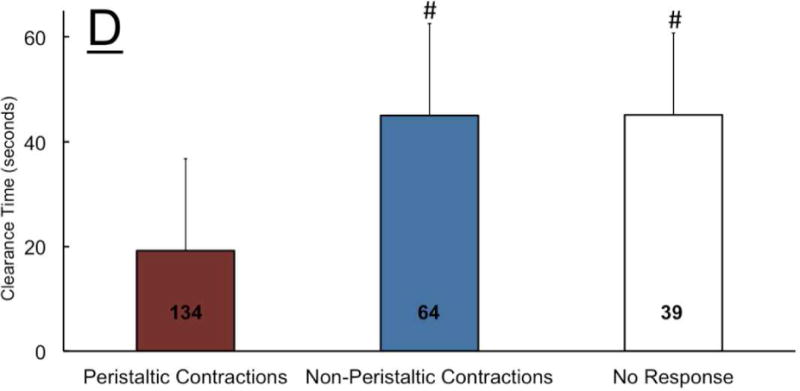
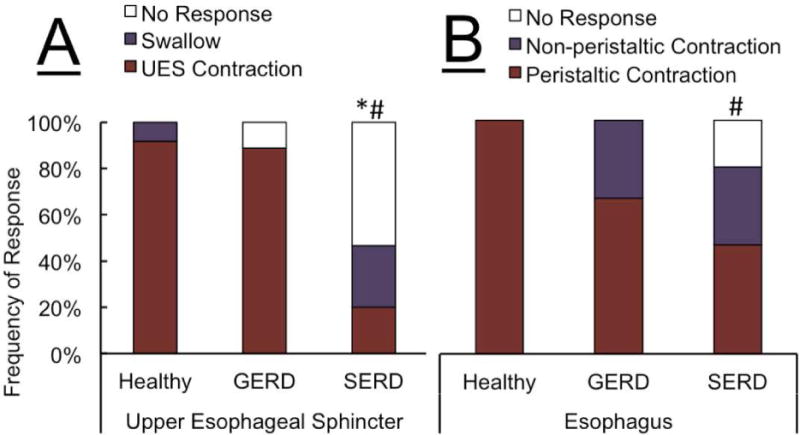
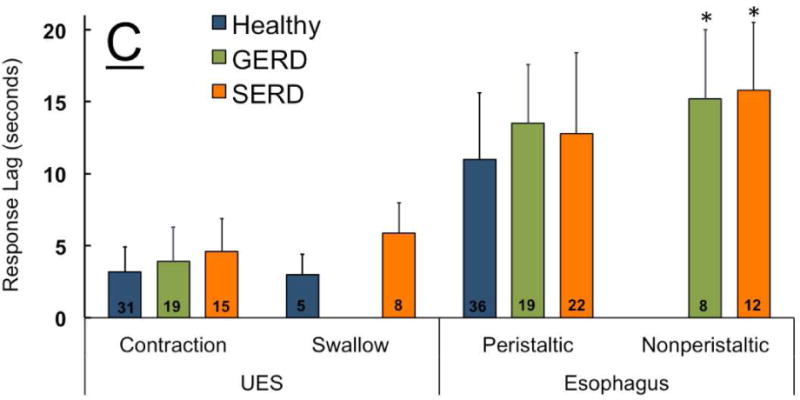
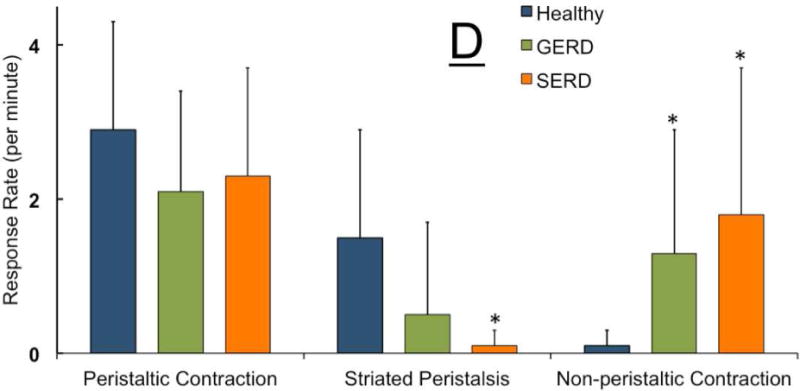
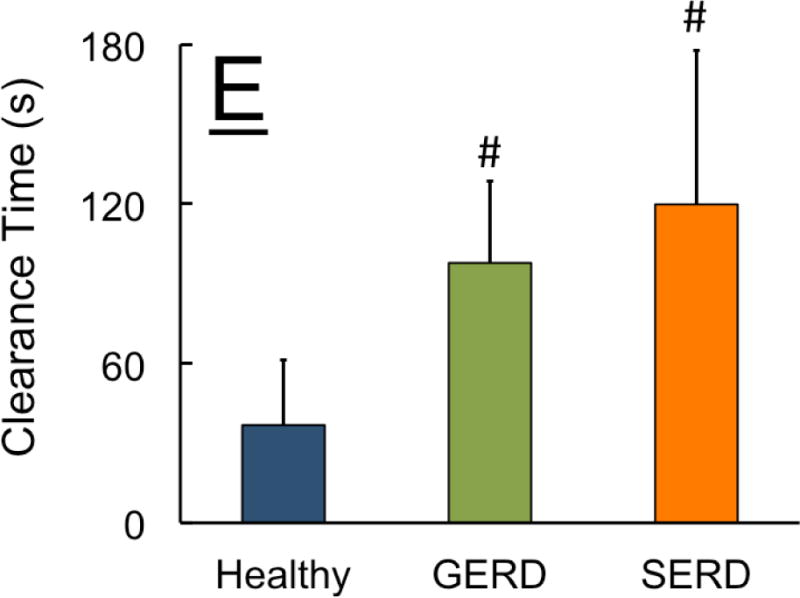
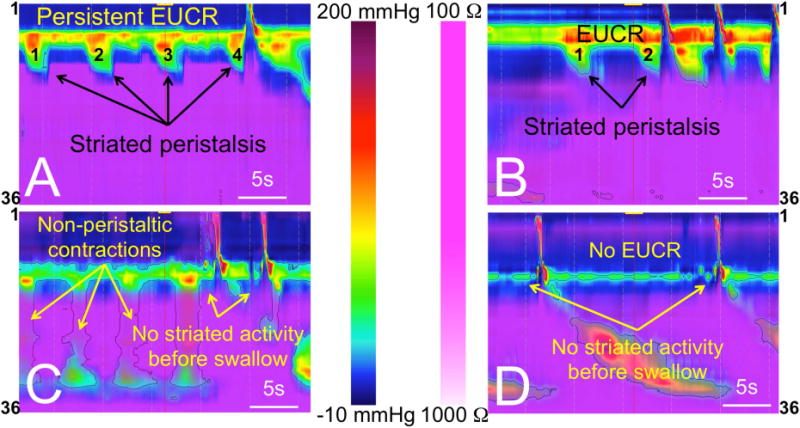
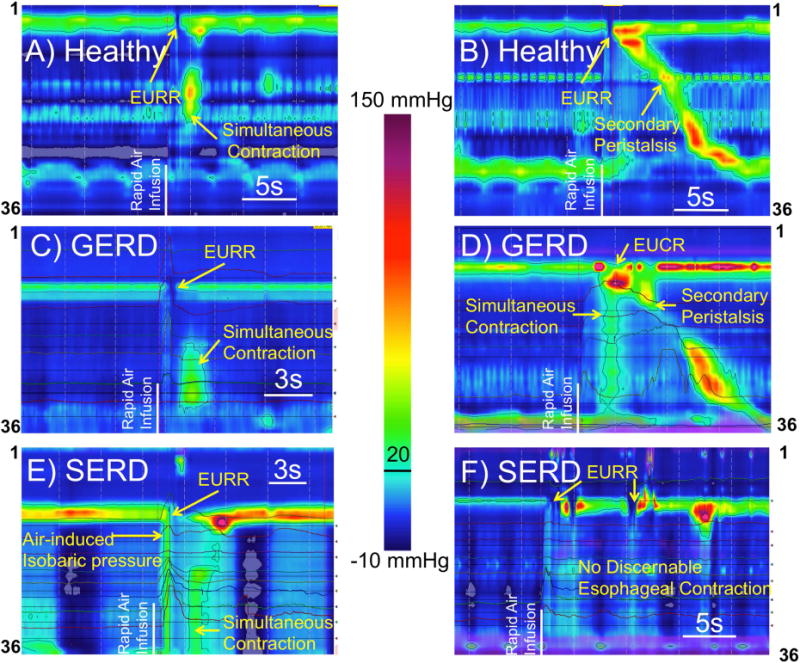
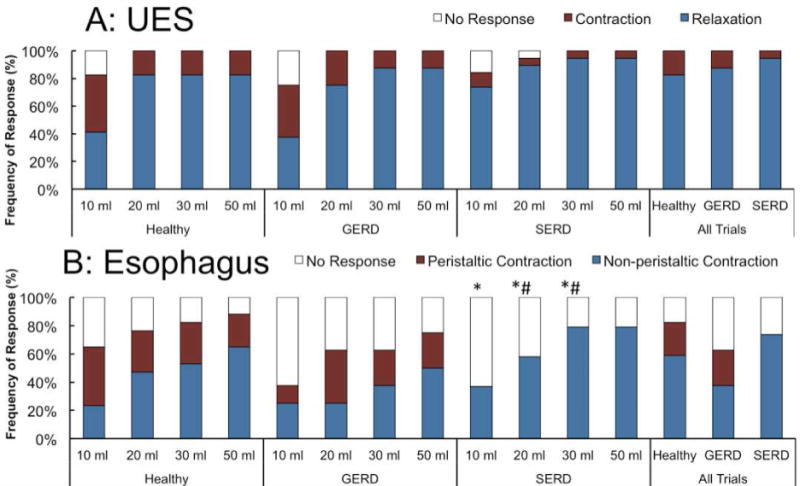
Results: A significantly smaller proportion of patients with SERD had UES contractile reflexes in response to slow esophageal infusion of acid than controls or patients with GERD. Only patients with SERD had abnormal UES relaxation responses to rapid distension with saline. Diminished esophageal peristaltic contractions resulted in esophageal stasis in patients with GERD or SERD.
Conclusions: Patients with SERD and complaints of regurgitation have impaired UES and esophageal responses to simulated liquid reflux events. These patterns could predispose them to esophagopharyngeal reflux.
Keywords: Cervical; EUCR; EURR; Extraesophageal Reflux; Laryngopharyngeal Reflux; Striated Esophagus.
Copyright © 2015 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors have no conflict of interest to disclose.
Figures
Comment in
-
Supraesophageal reflux disease: solving a riddle wrapped in a mystery inside an enigma.Gastroenterology. 2015 Nov;149(6):1318-20. doi: 10.1053/j.gastro.2015.09.033. Epub 2015 Sep 28. Gastroenterology. 2015. PMID: 26416325 No abstract available.
-
RE: Impaired Upper Esophageal Sphincter Reflexes in Patients With Supraesophageal Reflux Disease.Gastroenterology. 2016 Apr;150(4):1045. doi: 10.1053/j.gastro.2015.12.043. Gastroenterology. 2016. PMID: 26930017 No abstract available.
-
Reply.Gastroenterology. 2016 Jun;150(7):1693-1694. doi: 10.1053/j.gastro.2016.05.002. Epub 2016 May 13. Gastroenterology. 2016. PMID: 27183190 No abstract available.
References
-
- Creamer B, Schlegel J. Motor responses of the esophagus to distention. J Appl Physiol. 1957;10:498–504. - PubMed
-
- Meltzer SJ. Secondary peristalsis of the esophagus – a demonstration on a dog with a permanent esophageal fistula. Proc Soc Exper Biol & Med. 1906;3:35–37.
-
- Shaker R, Lang IM. Reflex mediated airway protective mechanisms against retrograde aspiration. The American journal of medicine. 1997;103:64S–73S. - PubMed
-
- Mearin F, Ponce J, Ponce M, et al. Frequency and clinical implications of supraesophageal and dyspeptic symptoms in gastroesophageal reflux disease. Eur J Gastroenterol Hepatol. 2012 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
