

Optical coherence tomography reflects brain atrophy in multiple sclerosis: A four-year study
- PMID: 26190464
- PMCID: PMC4703093
- DOI: 10.1002/ana.24487
Optical coherence tomography reflects brain atrophy in multiple sclerosis: A four-year study
Abstract
Objective: The aim of this work was to determine whether atrophy of specific retinal layers and brain substructures are associated over time, in order to further validate the utility of optical coherence tomography (OCT) as an indicator of neuronal tissue damage in patients with multiple sclerosis (MS).
Methods: Cirrus high-definition OCT (including automated macular segmentation) was performed in 107 MS patients biannually (median follow-up: 46 months). Three-Tesla magnetic resonance imaging brain scans (including brain-substructure volumetrics) were performed annually. Individual-specific rates of change in retinal and brain measures (estimated with linear regression) were correlated, adjusting for age, sex, disease duration, and optic neuritis (ON) history.
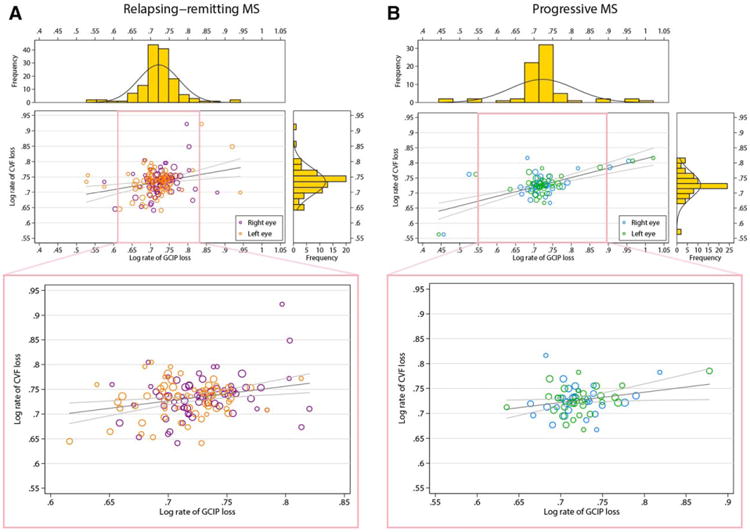
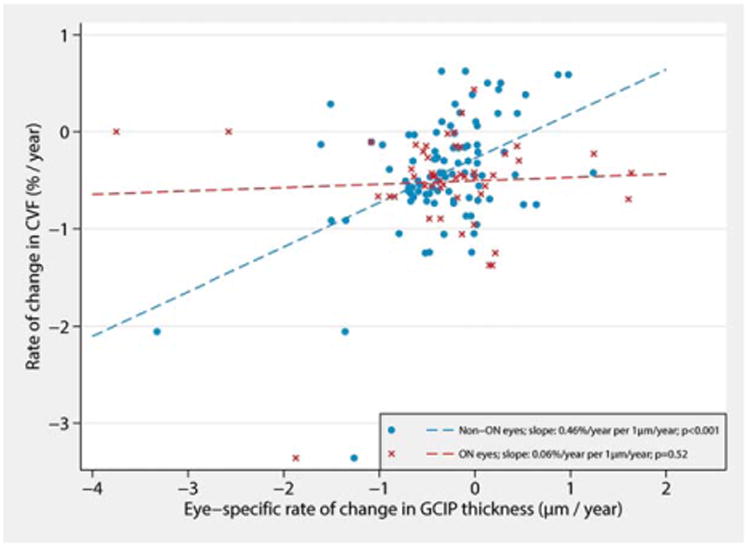
Results: Rates of ganglion cell + inner plexiform layer (GCIP) and whole-brain (r = 0.45; p < 0.001), gray matter (GM; r = 0.37; p < 0.001), white matter (WM; r = 0.28; p = 0.007), and thalamic (r = 0.38; p < 0.001) atrophy were associated. GCIP and whole-brain (as well as GM and WM) atrophy rates were more strongly associated in progressive MS (r = 0.67; p < 0.001) than relapsing-remitting MS (RRMS; r = 0.33; p = 0.007). However, correlation between rates of GCIP and whole-brain (and additionally GM and WM) atrophy in RRMS increased incrementally with step-wise refinement to exclude ON effects; excluding eyes and then patients (to account for a phenotype effect), the correlation increased to 0.45 and 0.60, respectively, consistent with effect modification. In RRMS, lesion accumulation rate was associated with GCIP (r = -0.30; p = 0.02) and inner nuclear layer (r = -0.25; p = 0.04) atrophy rates.
Interpretation: Over time GCIP atrophy appears to mirror whole-brain, and particularly GM, atrophy, especially in progressive MS, thereby reflecting underlying disease progression. Our findings support OCT for clinical monitoring and as an outcome in investigative trials.
© 2015 American Neurological Association.
Conflict of interest statement
Figures
References
-
- Kappos L, Moeri D, Radue EW, et al. Predictive value of gadolinium-enhanced magnetic resonance imaging for relapse rate and changes in disability or impairment in multiple sclerosis: A meta-analysis. Gadolinium MRI Meta-analysis Group. Lancet. 1999;353:964–969. - PubMed
-
- Fisher E, Rudick RA, Simon JH, et al. Eight-year follow-up study of brain atrophy in patients with MS. Neurology. 2002;59:1412–1420. - PubMed
-
- Sormani MP, Arnold DL, De Stefano N. Treatment effect on brain atrophy correlates with treatment effect on disability in multiple sclerosis. Ann Neurol. 2014;75:43–49. - PubMed
-
- van Waesberghe JH, Kamphorst W, De Groot CJ, et al. Axonal loss in multiple sclerosis lesions: magnetic resonance imaging insights into substrates of disability. Ann Neurol. 1999;46:747–754. - PubMed
-
- De Stefano N, Narayanan S, Francis GS, et al. Evidence of axonal damage in the early stages of multiple sclerosis and its relevance to disability. Arch Neurol. 2001;58:65–70. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
