

Intraductal papillary neoplasm of the bile duct, gastric type, arising in the intrapancreatic common bile duct could progress to colloid carcinoma: report of a case
- PMID: 26191308
- PMCID: PMC4503179
Intraductal papillary neoplasm of the bile duct, gastric type, arising in the intrapancreatic common bile duct could progress to colloid carcinoma: report of a case
Abstract
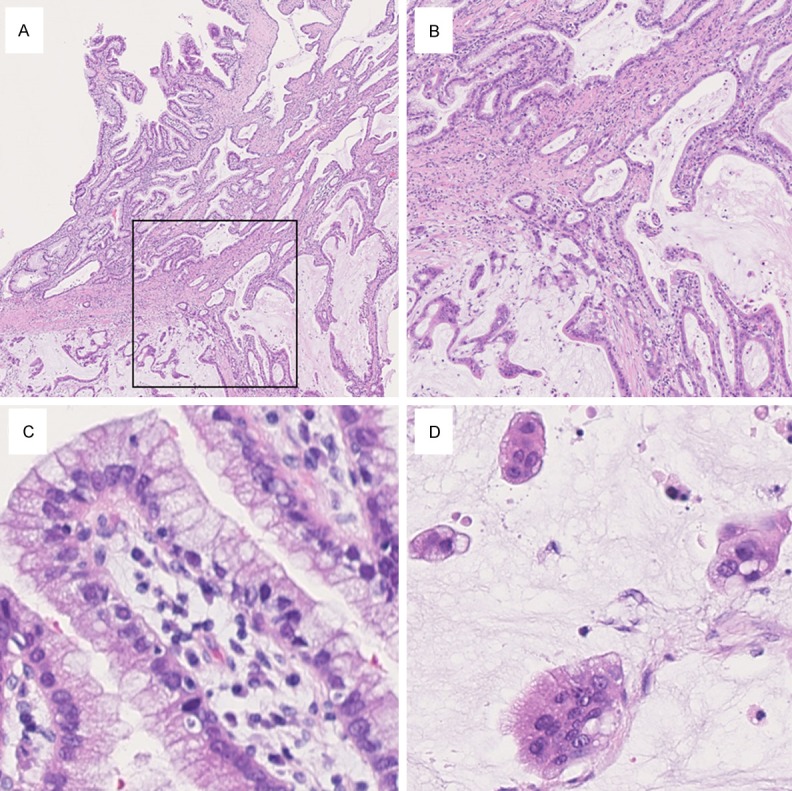
Intraductal papillary neoplasm of the bile duct (IPNB) exists in a pathway of multistep-carcinogenesis toward cholangiocarcinoma. Four subtypes are observed in IPNB, pancreatobiliary type, intestinal type, gastric type, and oncocytic type, similarly to the corresponding disease in the pancreas, intraductal papillary mucinous neoplasm (IPMN). IPNB can present with or without macroscopically visible mucin secretion. IPNB usually progresses to tubular adenocarcinoma. However, there are a limited number of well-described cases of gastric-type IPNB progressing not to tubular adenocarcinoma but to colloid carcinoma. Herein, we present a case of an 82-year-old female patient with gastric-type IPNB in the intrapancreatic common bile duct without macroscopically visible mucin secretion, which progressed to colloid carcinoma. As IPNB, especially without visible mucin secretion, is considered to be a heterogeneous group of diseases, such an unexpected association could occur.
Keywords: Intraductal papillary neoplasm of the bile duct; colloid carcinoma; gastric type; intraductal papillary mucinous neoplasm.
Figures



References
-
- Nakanuma Y, Sato Y, Ojima H, Kanai Y, Aishima S, Yamamoto M, Ariizumi S, Furukawa T, Hayashi H, Unno M, Ohta T Hepatolithiasis Subdivision of Intractable Hepatobiliary Diseases Study Group of Japan. Clinicopathological characterization of so-called “cholangiocarcinoma with intraductal papillary growth” with respect to “intraductal papillary neoplasm of bile duct (IPNB)”. Int J Clin Exp Pathol. 2014;7:3112–3122. - PMC - PubMed
-
- Nakanuma Y, Zen Y, Harada K, Ikeda H, Sato Y, Uehara T, Sasaki M. Tumorigenesis and phenotypic characteristics of mucin-producing bile duct tumors: an immunohistochemical approach. J Hepatobiliary Pancreat Sci. 2010;17:211–222. - PubMed
-
- Ohtsuka M, Kimura F, Shimizu H, Yoshidome H, Kato A, Yoshitomi H, Furukawa K, Takeuchi D, Takayashiki T, Suda K, Takano S, Kondo Y, Miyazaki M. Similarities and differences between intraductal papillary tumors of the bile duct with and without macroscopically visible mucin secretion. Am J Surg Pathol. 2011;35:512–521. - PubMed
-
- Kang GH, Moon HS, Lee ES, Kim SH, Sung JK, Lee B, Jeong HY. A case of colloid carcinoma arising in association with intraductal papillary neoplasm of the liver. Korean J Gastroenterol. 2012;60:386–390. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials