

A Direct Comparison of Three Clinically Relevant Treatments in a Rat Model of Cervical Spinal Cord Injury
- PMID: 26192071
- PMCID: PMC4638208
- DOI: 10.1089/neu.2015.3892
A Direct Comparison of Three Clinically Relevant Treatments in a Rat Model of Cervical Spinal Cord Injury
Abstract
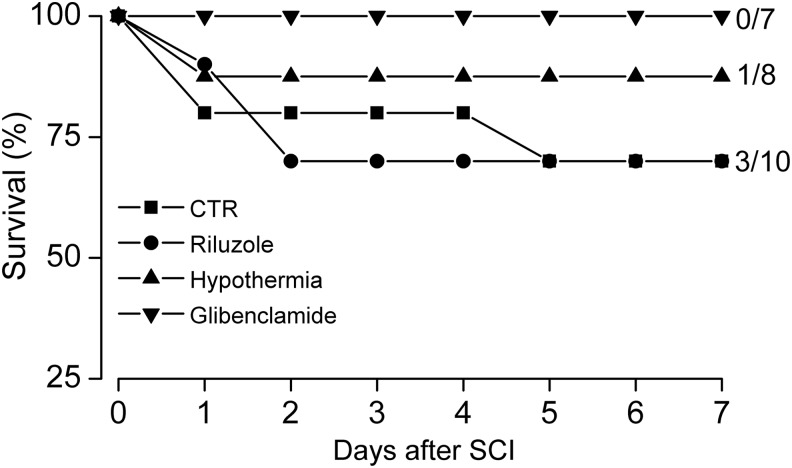
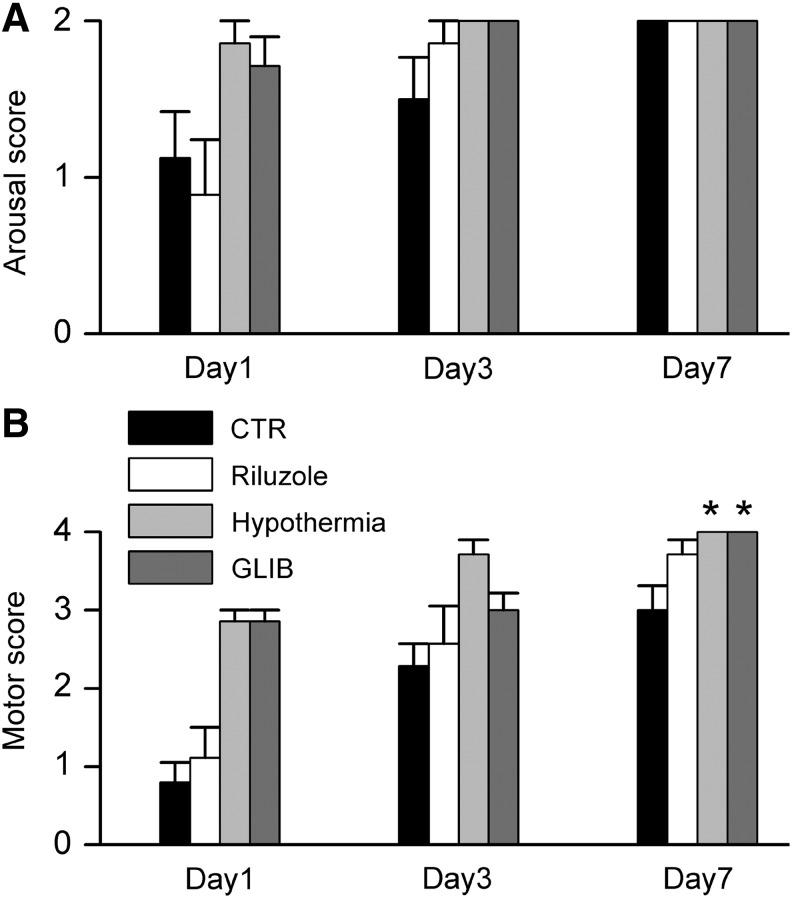
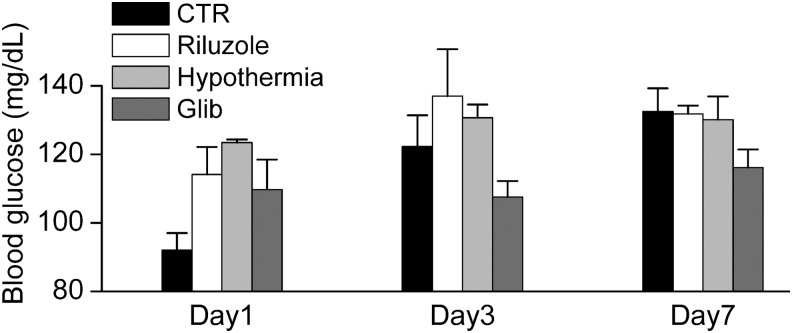
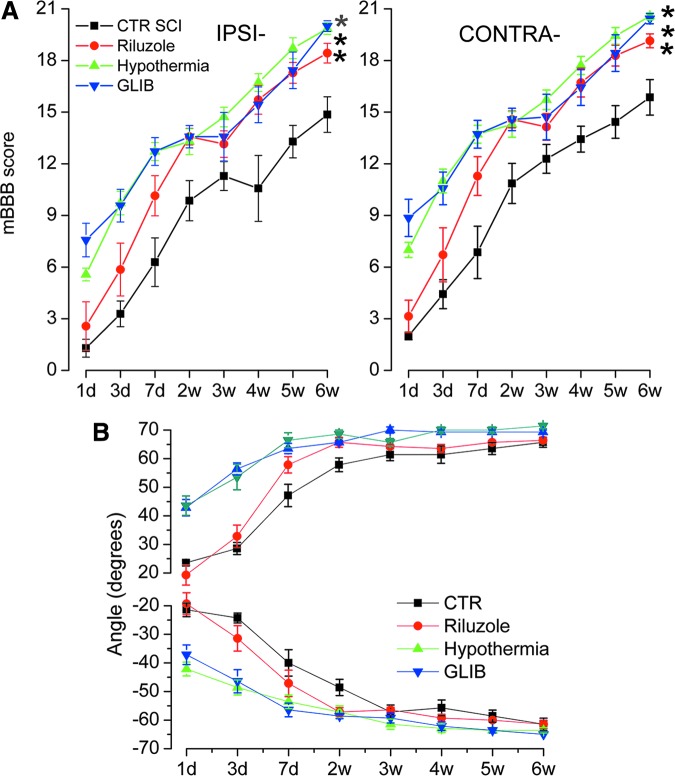
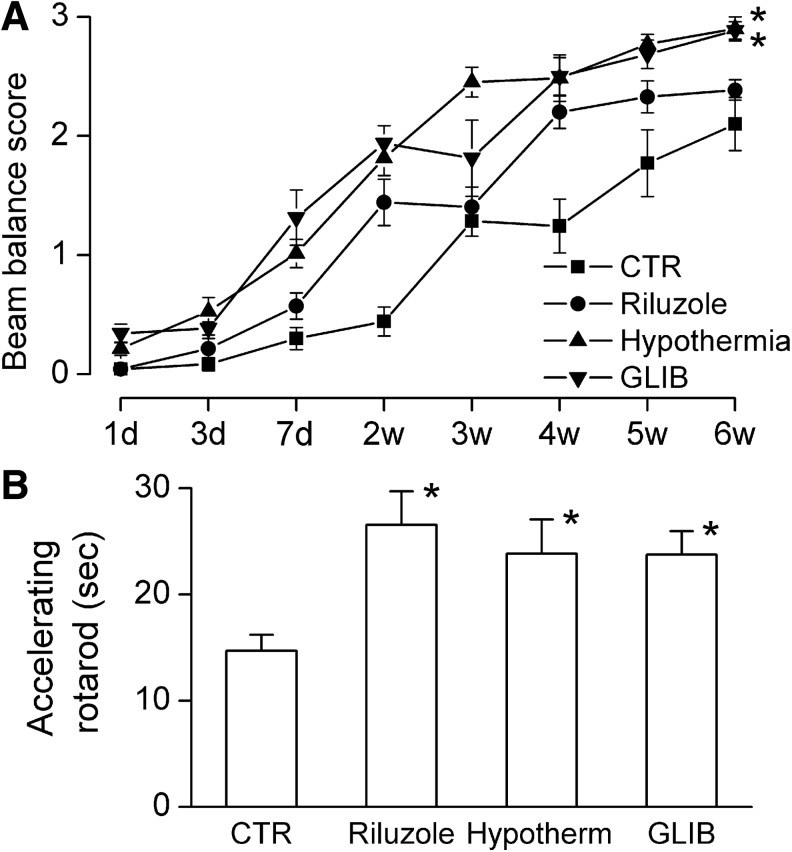
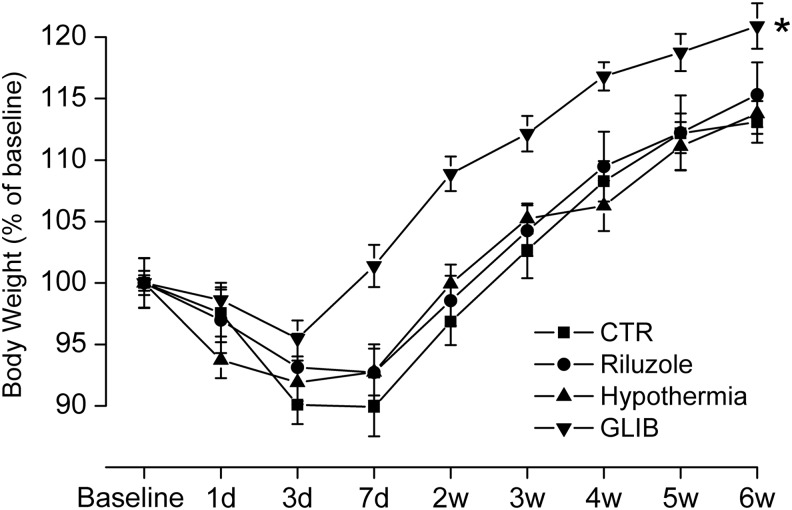
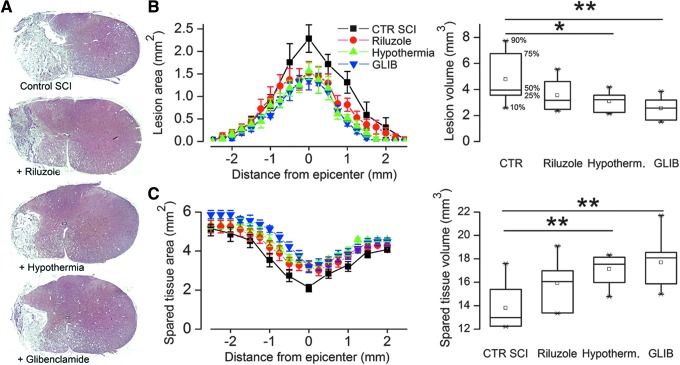
Recent preclinical studies have identified three treatments that are especially promising for reducing acute lesion expansion following traumatic spinal cord injury (SCI): riluzole, systemic hypothermia, and glibenclamide. Each has demonstrated efficacy in multiple studies with independent replication, but there is no way to compare them in terms of efficacy or safety, since different models were used, different laboratories were involved, and different outcomes were evaluated. Here, using a model of lower cervical hemicord contusion, we compared safety and efficacy for the three treatments, administered beginning 4 h after trauma. Treatment-associated mortality was 30% (3/10), 30% (3/10), 12.5% (1/8), and 0% (0/7) in the control, riluzole, hypothermia, and glibenclamide groups, respectively. For survivors, all three treatments showed overall favorable efficacy, compared with controls. On open-field locomotor scores (modified Basso, Beattie, and Bresnahan scores), hypothermia- and glibenclamide-treated animals were largely indistinguishable throughout the study, whereas riluzole-treated rats underperformed for the first two weeks; during the last four weeks, scores for the three treatments were similar, and significantly different from controls. On beam balance, hypothermia and glibenclamide treatments showed significant advantages over riluzole. After trauma, rats in the glibenclamide group rapidly regained a normal pattern of weight gain that differed markedly and significantly from that in all other groups. Lesion volumes at six weeks were: 4.8±0.7, 3.5±0.4, 3.1±0.3 and 2.5±0.3 mm(3) in the control, riluzole, hypothermia, and glibenclamide groups, respectively; measurements of spared spinal cord tissue confirmed these results. Overall, in terms of safety and efficacy, systemic hypothermia and glibenclamide were superior to riluzole.
Keywords: glibenclamide; hypothermia; rat; riluzole; spinal cord injury; sulfonylurea receptor 1 (Sur1).
Figures
Similar articles
-
Comparative effects of glibenclamide and riluzole in a rat model of severe cervical spinal cord injury.Exp Neurol. 2012 Jan;233(1):566-74. doi: 10.1016/j.expneurol.2011.11.044. Epub 2011 Dec 8. Exp Neurol. 2012. PMID: 22177998 Free PMC article.
-
Combining neuroprotective agents: effect of riluzole and magnesium in a rat model of thoracic spinal cord injury.Spine J. 2016 Aug;16(8):1015-24. doi: 10.1016/j.spinee.2016.04.013. Epub 2016 Apr 21. Spine J. 2016. PMID: 27109831
-
Effects of Therapeutic Hypothermia on Apoptosis and Autophagy After Spinal Cord Injury in Rats.Spine (Phila Pa 1976). 2015 Jun 15;40(12):883-90. doi: 10.1097/BRS.0000000000000845. Spine (Phila Pa 1976). 2015. PMID: 25705963
-
Efficacy of riluzole in the treatment of spinal cord injury: a systematic review of the literature.Neurosurg Focus. 2019 Mar 1;46(3):E6. doi: 10.3171/2019.1.FOCUS18596. Neurosurg Focus. 2019. PMID: 30835675
-
Systemic hypothermia for the treatment of acute cervical spinal cord injury in sports.Curr Sports Med Rep. 2011 Jan-Feb;10(1):50-4. doi: 10.1249/JSR.0b013e318205e0b3. Curr Sports Med Rep. 2011. PMID: 21228652 Review.
Cited by
-
A Direct Comparison of Physical Versus Dihydrocapsaicin-Induced Hypothermia in a Rat Model of Traumatic Spinal Cord Injury.Ther Hypothermia Temp Manag. 2022 Jun;12(2):90-102. doi: 10.1089/ther.2021.0013. Epub 2021 Oct 7. Ther Hypothermia Temp Manag. 2022. PMID: 35675523 Free PMC article.
-
Pediatric Spinal Cord Injury: A Review.Children (Basel). 2023 Aug 26;10(9):1456. doi: 10.3390/children10091456. Children (Basel). 2023. PMID: 37761417 Free PMC article. Review.
-
Assessment and management of acute spinal cord injury: From point of injury to rehabilitation.J Spinal Cord Med. 2017 Nov;40(6):665-675. doi: 10.1080/10790268.2017.1329076. Epub 2017 Jun 1. J Spinal Cord Med. 2017. PMID: 28571527 Free PMC article. Review.
-
Sulfonylurea Receptor 1 in Central Nervous System Injury: An Updated Review.Int J Mol Sci. 2021 Nov 2;22(21):11899. doi: 10.3390/ijms222111899. Int J Mol Sci. 2021. PMID: 34769328 Free PMC article. Review.
-
Promising neuroprotective strategies for traumatic spinal cord injury with a focus on the differential effects among anatomical levels of injury.F1000Res. 2017 Oct 30;6:1907. doi: 10.12688/f1000research.11633.1. eCollection 2017. F1000Res. 2017. PMID: 29152227 Free PMC article. Review.
References
-
- Wyndaele M. and Wyndaele J.J. (2006). Incidence, prevalence and epidemiology of spinal cord injury: what learns a worldwide literature survey? Spinal Cord. 44, 523–529 - PubMed
-
- Wyndaele J. J. (2011). More knowledge of worldwide incidence and epidemiology of spinal cord injury: data from the United States military. Spinal Cord. 49, 857. - PubMed
-
- Participants, Paralysis Consensus Conference, Christopher and Dana Reeve Foundation. One degree of separation; paralysis and spinal cord injury in the United States. Christopher and Dana Reeve Foundation 2014 December 5; Available at: www.christopherreeve.org/atf/cf/%7B3d83418f-b967-4c18-8ada-adc2e5355071%... Accessed June21, 2015
-
- Spinal cord injury (SCI) fact sheet. Centers for Disease Prevention and Control 2014 December 5; Available at: http://manoa.hawaii.edu/pbrrtc/wp-content/uploads/2014/12/SpinalCordInju... Accessed December5, 2014
-
- Schoenfeld A. J., Sielski B., Rivera K.P., Bader J.O., and Harris M.B. (2012). Epidemiology of cervical spine fractures in the US military. Spine J. 12, 777–783 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical