

Can Confirmatory Biopsy be Omitted in Patients with Prostate Cancer Favorable Diagnostic Features on Active Surveillance?
- PMID: 26192258
- PMCID: PMC4840176
- DOI: 10.1016/j.juro.2015.07.078
Can Confirmatory Biopsy be Omitted in Patients with Prostate Cancer Favorable Diagnostic Features on Active Surveillance?
Abstract
Purpose: We evaluated whether initial diagnostic parameters could predict the confirmatory biopsy result in patients initiating active surveillance for prostate cancer, to determine whether some men at low risk for disease reclassification could be spared unnecessary biopsy.
Materials and methods: The cohort included 392 men with Gleason 6 prostate cancer on initial biopsy undergoing confirmatory biopsy. We used univariate and multivariable logistic regression to assess if high grade cancer (Gleason 7 or greater) on confirmatory biopsy could be predicted from initial diagnostic parameters (prostate specific antigen density, magnetic resonance imaging result, percent positive cores, percent cancer in positive cores and total tumor length).
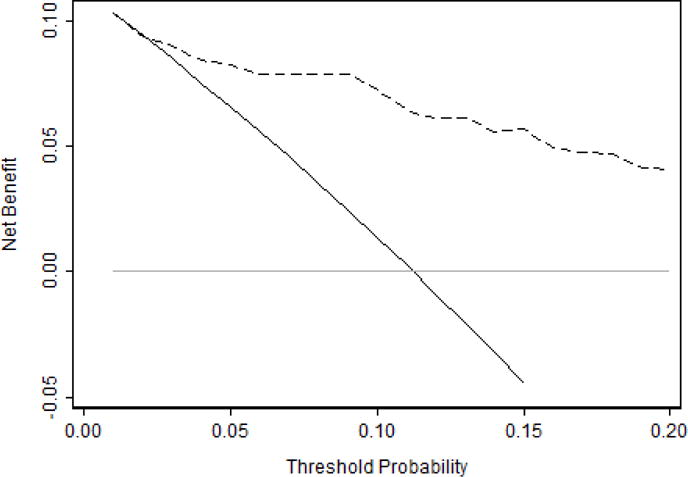
Results: Median patient age was 62 years (IQR 56-66) and 47% of patients had a dominant or focal lesion on magnetic resonance imaging. Of the 392 patients 44 (11%) had high grade cancer on confirmatory biopsy, of whom 39 had Gleason 3+4, 1 had 4+3, 3 had Gleason 8 and 1 had Gleason 9 disease. All predictors were significantly associated with high grade cancer at confirmatory biopsy on univariate analysis. However, in the multivariable model only prostate specific antigen density and total tumor length were significantly associated (AUC 0.85). Using this model to select patients for confirmatory biopsy would generally provide a higher net benefit than performing confirmatory biopsy in all patients, across a wide range of threshold probabilities.
Conclusions: If externally validated, a model based on initial diagnostic criteria could be used to avoid confirmatory biopsy in many patients initiating active surveillance.
Keywords: biopsy; prostatic neoplasms; watchful waiting.
Copyright © 2016 American Urological Association Education and Research, Inc. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Prostate cancer: Avoiding excess confirmatory biopsies.Nat Rev Urol. 2015 Sep;12(9):476. doi: 10.1038/nrurol.2015.195. Epub 2015 Aug 4. Nat Rev Urol. 2015. PMID: 26238030 No abstract available.
-
How Often is Biopsy Necessary in Patients with Prostate Cancer on Active Surveillance?J Urol. 2016 Jan;195(1):11-2. doi: 10.1016/j.juro.2015.10.061. Epub 2015 Oct 19. J Urol. 2016. PMID: 26475660 No abstract available.
References
-
- Mohler JL, Armstrong AJ, Bahson RR, et al. National Comprehensive Cancer Network guidelines: prostate cancer version 1.2015. http://www.nccn.org/professionals/physician_gls/pdf/prostate.pdf. Published October 24, 2014. Accessed April 17, 2015.
-
- Mottet N, Bellmunt J, Briers E, et al. European Association of Urology guidelines on prostate cancer (March 2015 update) http://uroweb.org/guideline/prostate-cancer/. Accessed April 17, 2015.
-
- Thompson I, Thrasher JB, Aus G, et al. American Urological Association guideline for the management of clinically localized prostate cancer. 2007 https://www.auanet.org/education/guidelines/prostate-cancer.cfm. Accessed April 17, 2015. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
