

Normal Perceptual Sensitivity Arising From Weakly Reflective Cone Photoreceptors
- PMID: 26193919
- PMCID: PMC4509056
- DOI: 10.1167/iovs.15-16547
Normal Perceptual Sensitivity Arising From Weakly Reflective Cone Photoreceptors
Abstract
Purpose: To determine the light sensitivity of poorly reflective cones observed in retinas of normal subjects, and to establish a relationship between cone reflectivity and perceptual threshold.
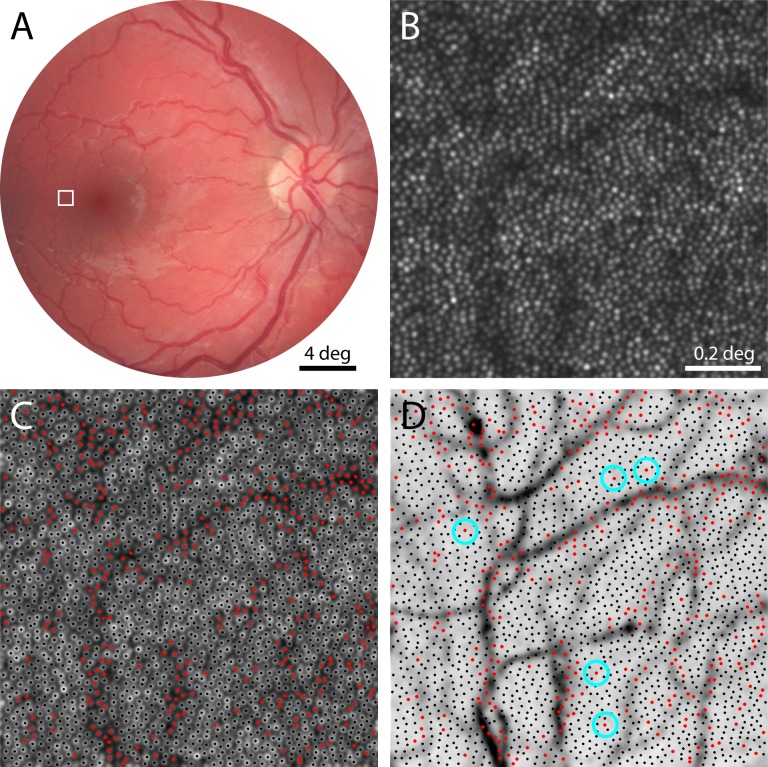
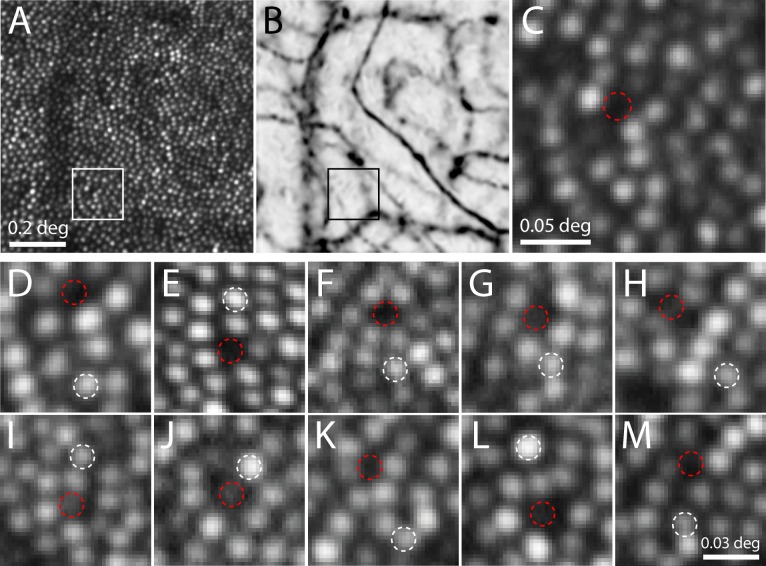
Methods: Five subjects (four male, one female) with normal vision were imaged longitudinally (7-26 imaging sessions, representing 82-896 days) using adaptive optics scanning laser ophthalmoscopy (AOSLO) to monitor cone reflectance. Ten cones with unusually low reflectivity, as well as 10 normally reflective cones serving as controls, were targeted for perceptual testing. Cone-sized stimuli were delivered to the targeted cones and luminance increment thresholds were quantified. Thresholds were measured three to five times per session for each cone in the 10 pairs, all located 2.2 to 3.3° from the center of gaze.
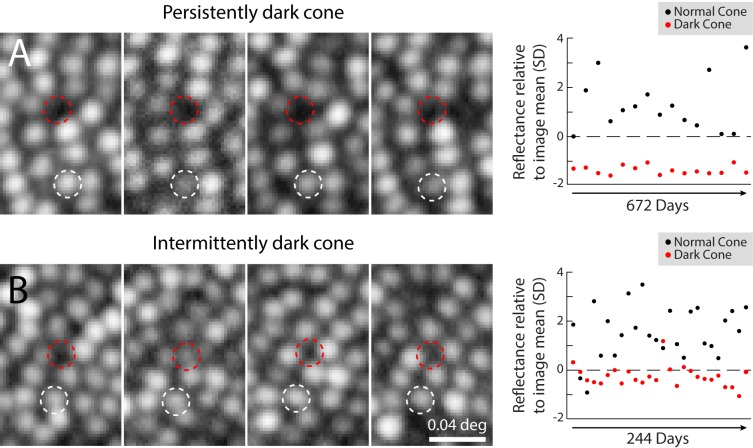
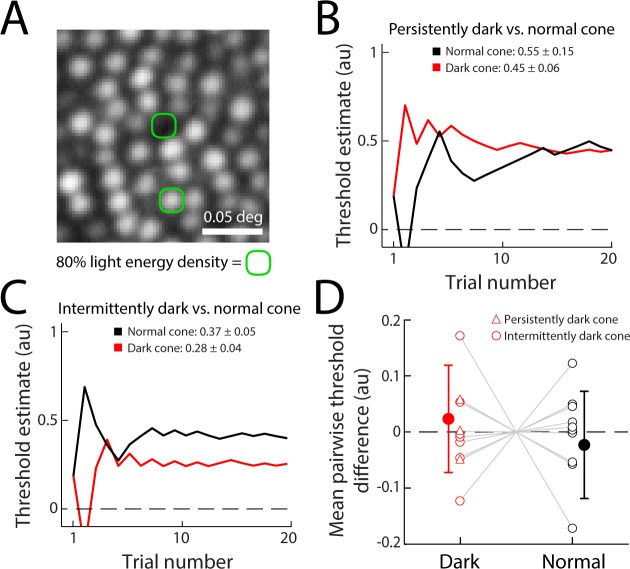
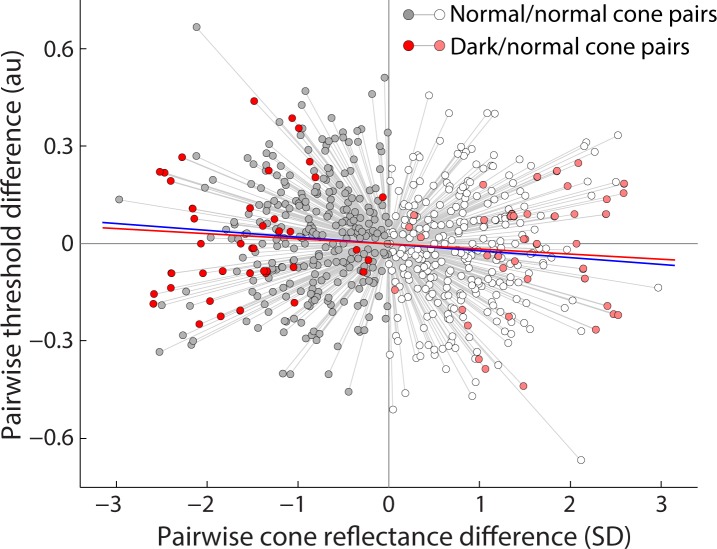
Results: Compared with other cones in the same retinal area, three of 10 monitored dark cones were persistently poorly reflective, while seven occasionally manifested normal reflectance. Tested psychophysically, all 10 dark cones had thresholds comparable with those from normally reflecting cones measured concurrently (P = 0.49). The variation observed in dark cone thresholds also matched the wide variation seen in a large population (n = 56 cone pairs, six subjects) of normal cones; in the latter, no correlation was found between cone reflectivity and threshold (P = 0.0502).
Conclusions: Low cone reflectance cannot be used as a reliable indicator of cone sensitivity to light in normal retinas. To improve assessment of early retinal pathology, other diagnostic criteria should be employed along with imaging and cone-based microperimetry.
Figures
References
-
- Lombardo M,, Parravano M,, Lombardo G,, et al. Adaptive optics imaging of parafoveal cones in type 1 diabetes. Retina. 2014; 34: 546–557. - PubMed
Publication types
MeSH terms
Grants and funding
- EY014375/EY/NEI NIH HHS/United States
- EY022412/EY/NEI NIH HHS/United States
- EY007043/EY/NEI NIH HHS/United States
- L30 EY021930/EY/NEI NIH HHS/United States
- R21 EY021642/EY/NEI NIH HHS/United States
- R01 EY023591/EY/NEI NIH HHS/United States
- F32 EY007043/EY/NEI NIH HHS/United States
- R01 EY023581/EY/NEI NIH HHS/United States
- P30 EY003039/EY/NEI NIH HHS/United States
- T35HL07473/HL/NHLBI NIH HHS/United States
- EY023591/EY/NEI NIH HHS/United States
- K23 EY022412/EY/NEI NIH HHS/United States
- EY003039/EY/NEI NIH HHS/United States
- T35 HL007473/HL/NHLBI NIH HHS/United States
- EY021642/EY/NEI NIH HHS/United States
- R01 EY014375/EY/NEI NIH HHS/United States
- T32 EY007043/EY/NEI NIH HHS/United States
- EY023581/EY/NEI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
