

The Alzheimer's Disease Neuroimaging Initiative 2 Biomarker Core: A review of progress and plans
- PMID: 26194312
- PMCID: PMC5127404
- DOI: 10.1016/j.jalz.2015.05.003
The Alzheimer's Disease Neuroimaging Initiative 2 Biomarker Core: A review of progress and plans
Abstract
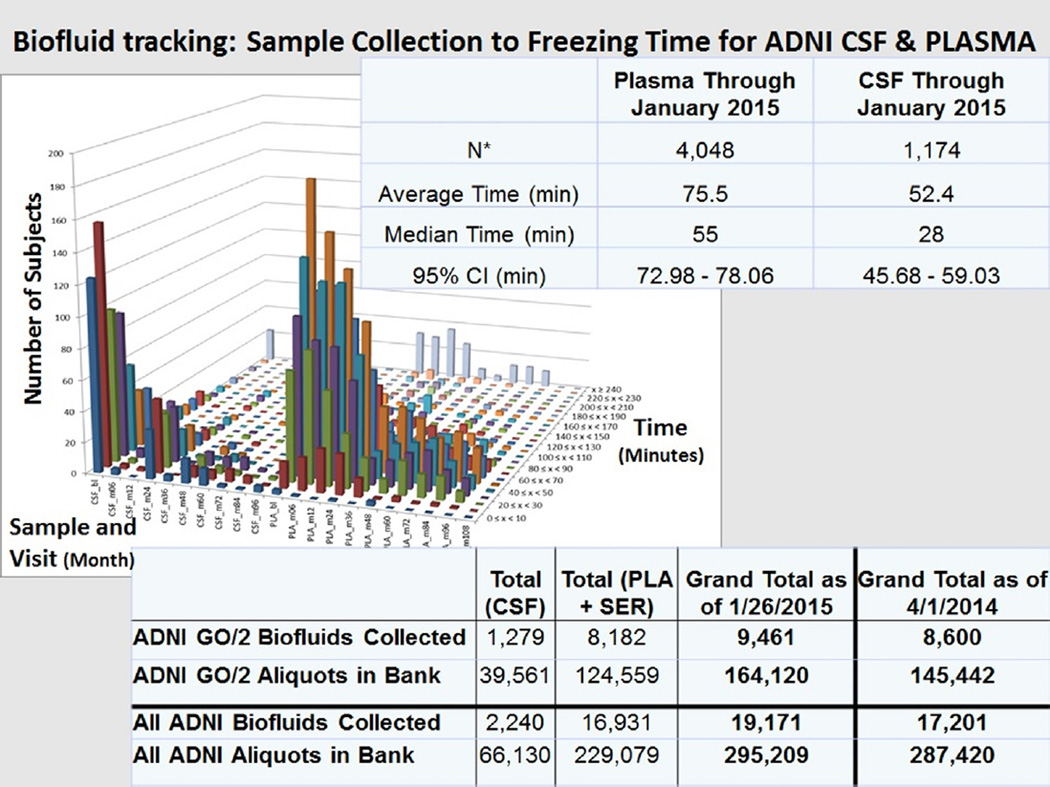
Introduction: We describe Alzheimer's Disease Neuroimaging Initiative (ADNI) Biomarker Core progress including: the Biobank; cerebrospinal fluid (CSF) amyloid beta (Aβ1-42), t-tau, and p-tau181 analytical performance, definition of Alzheimer's disease (AD) profile for plaque, and tangle burden detection and increased risk for progression to AD; AD disease heterogeneity; progress in standardization; and new studies using ADNI biofluids.
Methods: Review publications authored or coauthored by ADNI Biomarker core faculty and selected non-ADNI studies to deepen the understanding and interpretation of CSF Aβ1-42, t-tau, and p-tau181 data.
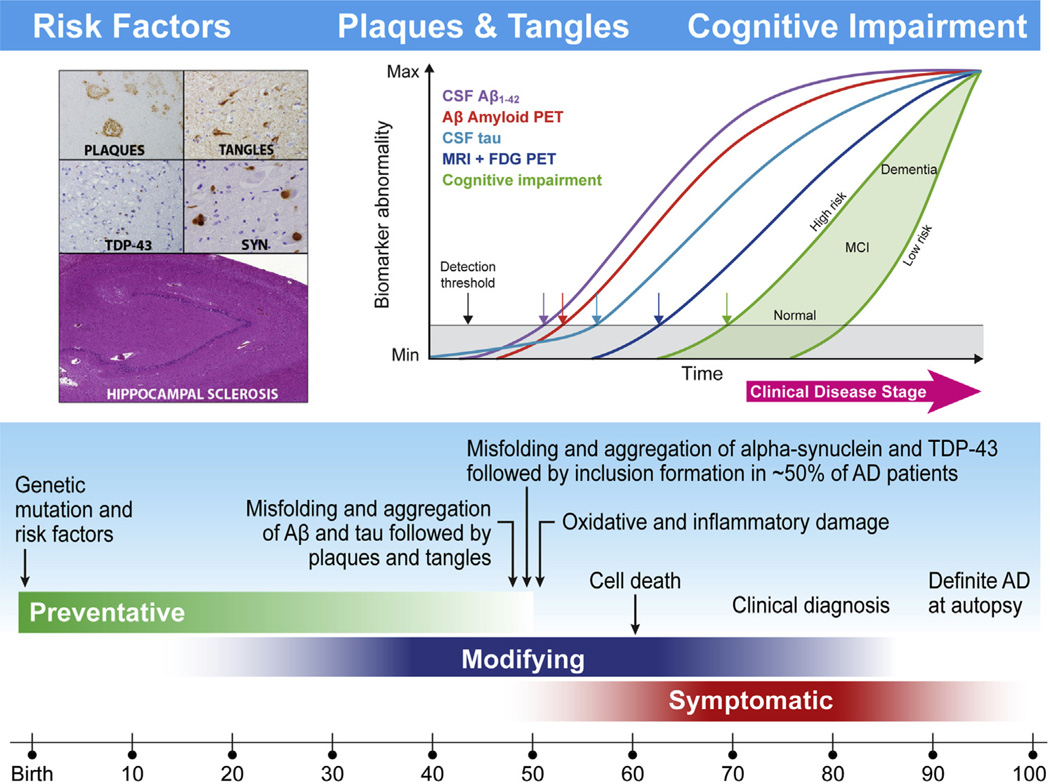
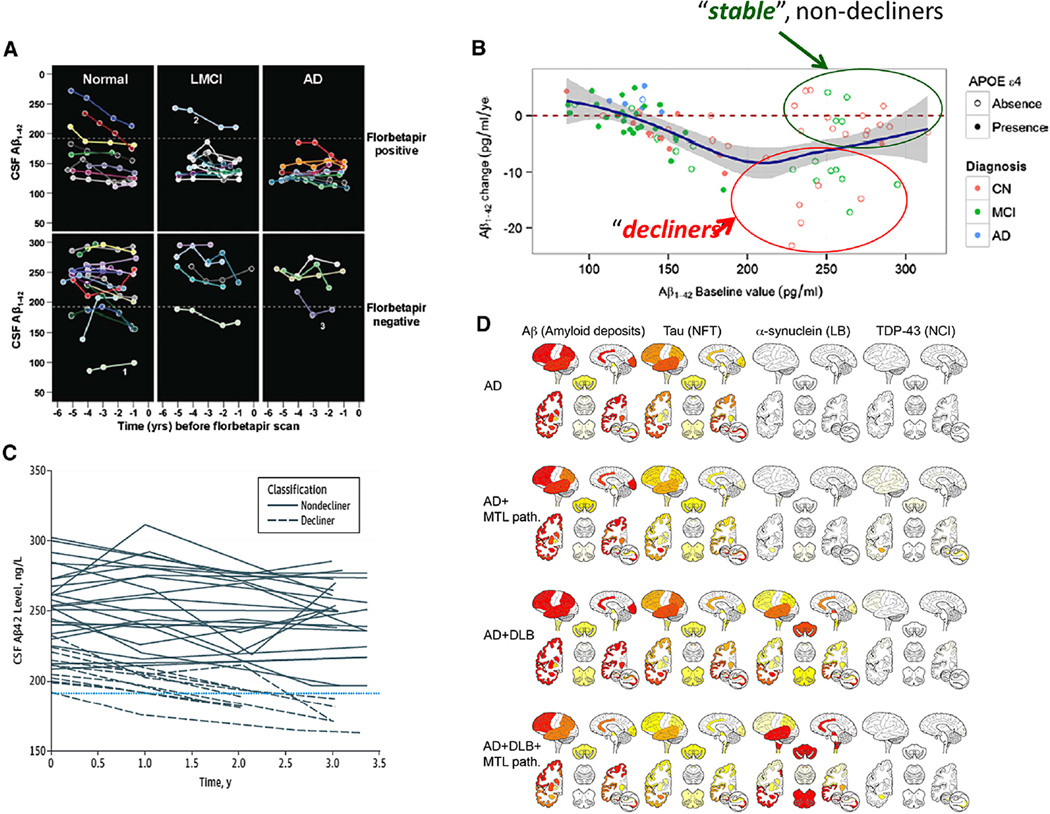
Results: CSF AD biomarker measurements with the qualified AlzBio3 immunoassay detects neuropathologic AD hallmarks in preclinical and prodromal disease stages, based on CSF studies in non-ADNI living subjects followed by the autopsy confirmation of AD. Collaboration across ADNI cores generated the temporal ordering model of AD biomarkers varying across individuals because of genetic/environmental factors that increase/decrease resilience to AD pathologies.
Discussion: Further studies will refine this model and enable the use of biomarkers studied in ADNI clinically and in disease-modifying therapeutic trials.
Keywords: ADNI; Alzheimer's disease; Aβ(1–42); Biomarkers; Cerebrospinal fluid; Disease-modifying therapy; Immunoassay; Mild cognitive impairment; Plasma; Tau.
Copyright © 2015. Published by Elsevier Inc.
Figures
References
-
- Schneider JA, Arvanitakis Z, Bang W, Bennett DA. Mixed brain pathologies account for most dementia cases in community-dwelling older persons. Neurology. 2007;69:2197–2204. - PubMed
-
- White L, Small BJ, Petrovitch H, Ross GW, Masaki K, Abbott RD, et al. Recent clinical-pathologic research on the causes of dementia in late life: update from the Honolulu-Asia Aging Study. J Geriatr Psychiatry Neurol. 2005;18:224–227. - PubMed
-
- Gomez-Isla T, Hollister R, West H, Mui S, Growdon JH, Petersen RC, et al. Neuronal loss correlates with but exceeds neurofibrillary tangles in Alzheimer’s disease. Ann Neurol. 1997;41:17–24. - PubMed
-
- Savva GM, Wharton SB, Ince PG, Forster G, Matthews FE, Brayne C, et al. Age, neuropathology, and dementia. N Engl J Med. 2009;360:2302–2309. - PubMed
-
- Terry RD, Masliah E, Salmon DP, Butters N, DeTeresa R, Hill R, et al. Physical basis of cognitive alterations in Alzheimer’s disease: synapse loss is the major correlate of cognitive impairment. Ann Neurol. 1991;30:572–580. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
