

Experimental Sleep Restriction Facilitates Pain and Electrically Induced Cortical Responses
- PMID: 26194577
- PMCID: PMC4576335
- DOI: 10.5665/sleep.5058
Experimental Sleep Restriction Facilitates Pain and Electrically Induced Cortical Responses
Abstract
Study objectives: Sleep restriction (SR) has been hypothesized to sensitize the pain system. The current study determined whether experimental sleep restriction had an effect on experimentally induced pain and pain-elicited electroencephalographic (EEG) responses.
Design: A paired crossover study.
Intervention: Pain testing was performed after 2 nights of 50% SR and after 2 nights with habitual sleep (HS).
Setting: Laboratory experiment at research center.
Participants: Self-reported healthy volunteers (n = 21, age range: 18-31 y).
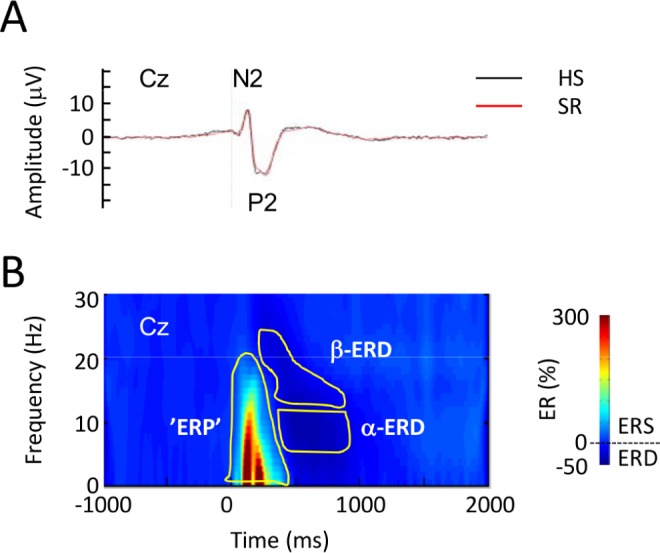
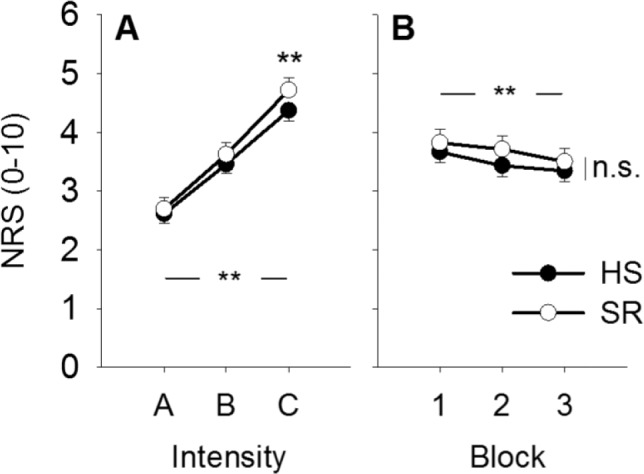
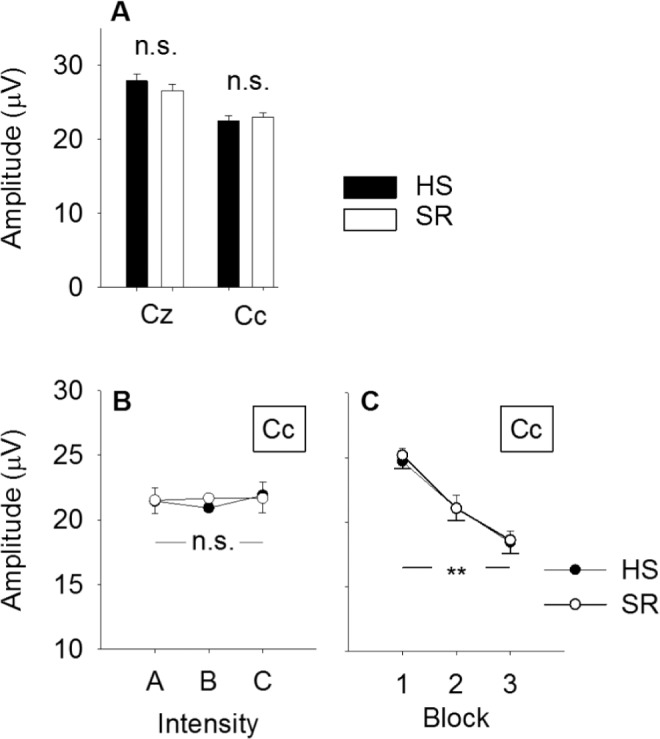
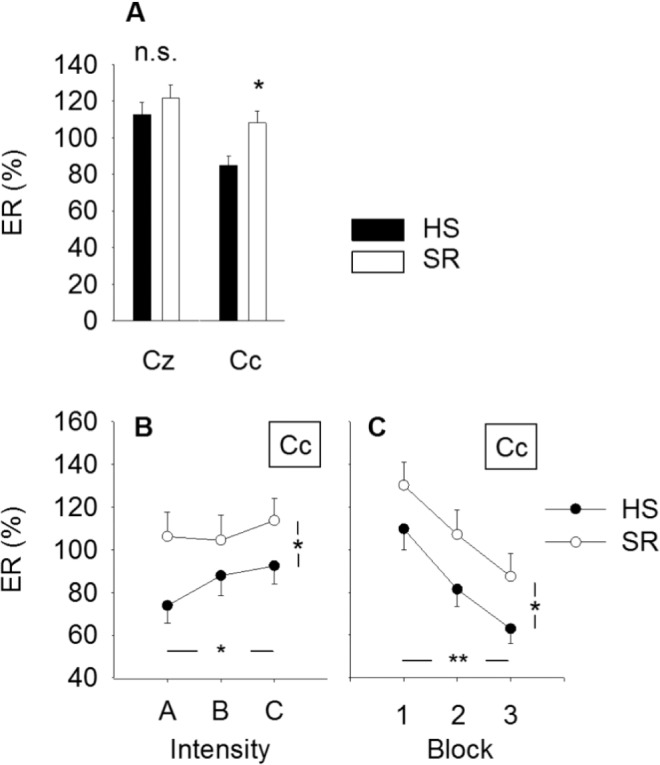
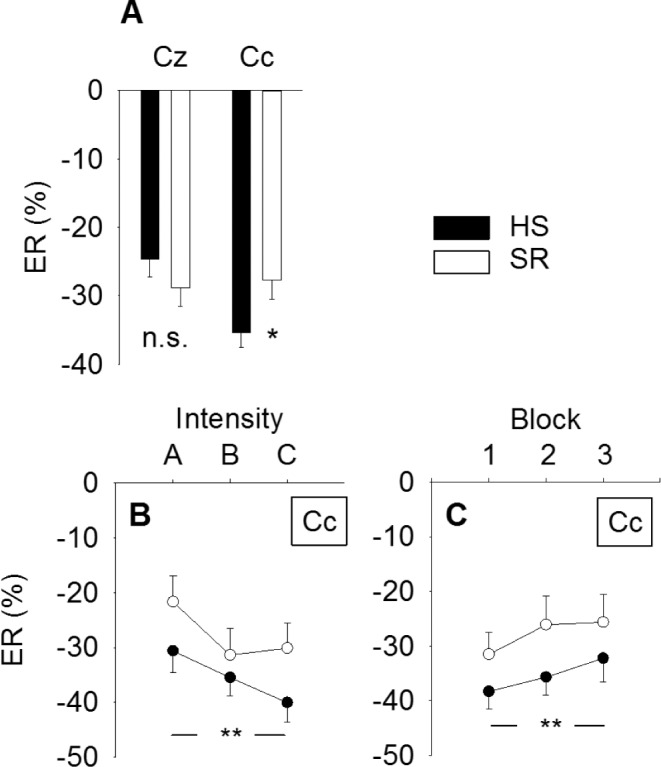
Measurements and results: Brief high-density electrical stimuli to the forearm skin produced pinprick-like pain. Subjective pain ratings increased after SR, but only in response to the highest stimulus intensity (P = 0.018). SR increased the magnitude of the pain-elicited EEG response analyzed in the time-frequency domain (P = 0.021). Habituation across blocks did not differ between HS and SR. Event-related desynchronization (ERD) was reduced after SR (P = 0.039). Pressure pain threshold of the trapezius muscle region also decreased after SR (P = 0.017).
Conclusion: Sleep restriction (SR) increased the sensitivity to pressure pain and to electrically induced pain of moderate, but not low, intensity. The increased electrical pain could not be explained by a difference in habituation. Increased response magnitude is possibly related to reduced processing within the somatosensory cortex after partial SR.
Keywords: EEG; event-related desynchronization (ERD); event-related potential (ERP); pain; pressure pain threshold (PPT); time-frequency analysis.
© 2015 Associated Professional Sleep Societies, LLC.
Figures
References
-
- Sivertsen B, Krokstad S, Overland S, Mykletun A. The epidemiology of insomnia: associations with physical and mental health. The HUNT-2 study. J Psychosom Res. 2009;67:109–16. - PubMed
-
- Uhlig BL, Sand T, Odegard SS, Hagen K. Prevalence and associated factors of DSM-V insomnia in Norway: the Nord-Trondelag Health Study (HUNT 3) Sleep Med. 2014;15:708–13. - PubMed
-
- Kaila-Kangas L, Kivimaki M, Harma M, et al. Sleep disturbances as predictors of hospitalization for back disorders-a 28-year follow-up of industrial employees. Spine (Phila Pa 1976) 2006;31:51–6. - PubMed
-
- Siivola SM, Levoska S, Latvala K, Hoskio E, Vanharanta H, Keinanen-Kiukaanniemi S. Predictive factors for neck and shoulder pain: a longitudinal study in young adults. Spine (Phila Pa 1976) 2004;29:1662–9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
