

Paravesical gossypiboma following inguinal herniorrhaphy: Laparoscopic retrieval
- PMID: 26195885
- PMCID: PMC4499932
- DOI: 10.4103/0972-9941.152099
Paravesical gossypiboma following inguinal herniorrhaphy: Laparoscopic retrieval
Abstract
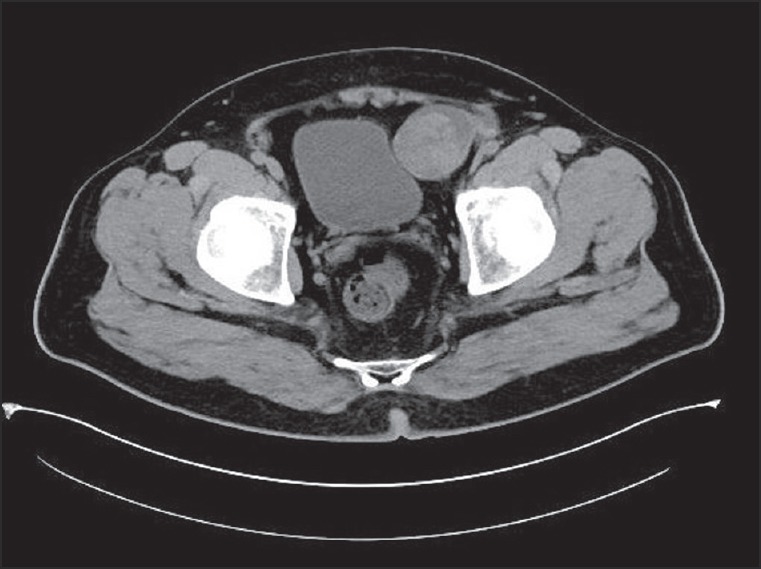
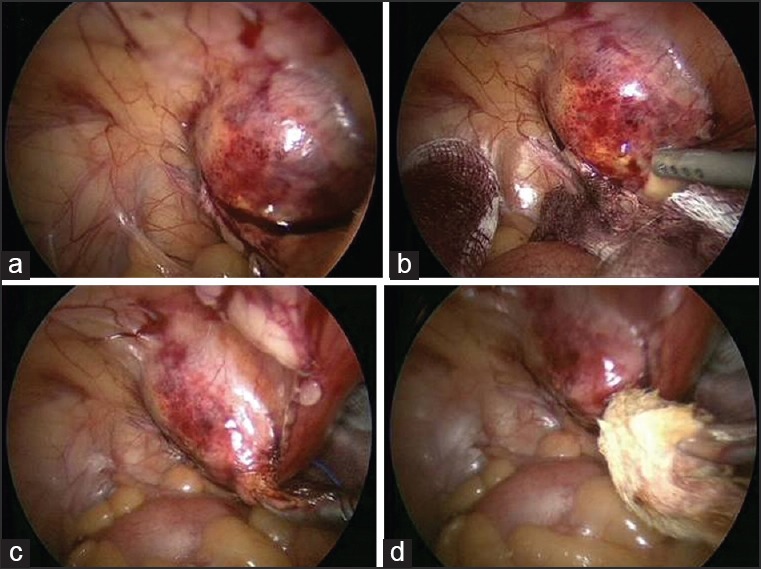
Retained surgical sponge (gossypiboma) following an inguinal herniorrhaphy is a rare condition and may cause medicolegal problems. Differential diagnosis for the lesion should be made meticulously. We report a case of a 45-year-old man who had a herniorrhaphy about 8 years previously. He presented one episode of painless gross hematuria. Laboratory and imaging studies excluded any significant lesion in the urological organs. Abdominal CT scan demonstrated a heterogeneous neoplasm of 4 cm in size in the left paravesical area that was retrieved laparoscopically. Abdominal CT and clinical suspicion are helpful for diagnosis. Laparoscopy may be used to confirm the diagnosis and to remove the retained surgical gauze, and considered as an alternative therapy for some selected patients.
Keywords: Gossypiboma; herniorrhaphy; laparoscopy.
Conflict of interest statement
Figures
References
-
- Gawande AA, Studdert DM, Orav EJ, Brennan TA, Zinner MJ. Risk factors for retained instruments and sponges after surgery. N Engl J Med. 2003;348:229–35. - PubMed
-
- Lauwers PR, Van Hee RH. Intraperitoneal gossypibomas: The need to count sponges. World J Surg. 2000;24:521–7. - PubMed
-
- Târcoveanu E, Dimofte G, Georgescu S, Vasilescu A, Lupaşcu C, Bradea C, et al. Laparoscopic retrieval of gossypibomas - short series and review of literature. Acta Chir Belg. 2011;111:366–9. - PubMed
-
- Rappaport W, Haynes K. The retained surgical sponge following intra-abdominal surgery: A continuing problem. Arch Surg. 1990;125:405–7. - PubMed
-
- Erdil A, Kilciler G, Ates Y, Tuzun A, Gulsen M, Karaeren N, et al. Transgastric migration of retained intraabdominal surgical sponge: Gossypiboma in the bulbus. Intern Med. 2008;47:613–5. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources