

A Cluster Randomized Controlled Trial of Nonpharmacological Interventions for Old-Old Subjects with a Clinical Dementia Rating of 0.5: The Kurihara Project
- PMID: 26195978
- PMCID: PMC4483494
- DOI: 10.1159/000380816
A Cluster Randomized Controlled Trial of Nonpharmacological Interventions for Old-Old Subjects with a Clinical Dementia Rating of 0.5: The Kurihara Project
Abstract
Background: Evidence as to the benefits of nonpharmacological interventions for the boundary state between normal aging and dementia [mild cognitive impairment or a Clinical Dementia Rating (CDR) of 0.5] remains weak due to a lack of positive controls.
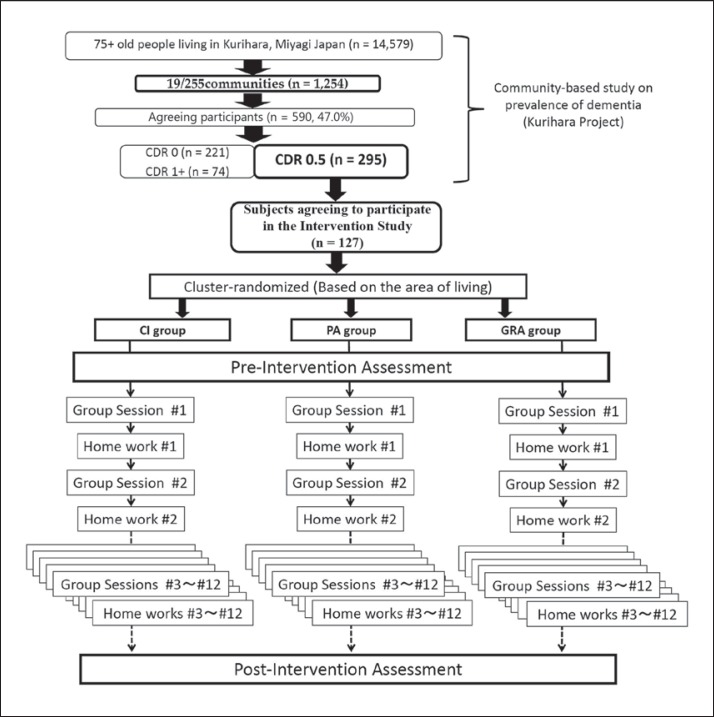
Aims: To directly compare the effects of cognitive interventions (CI), physical activities (PA) and a group reminiscence approach (GRA), we conducted a pilot study on the basis of a cluster randomized controlled trial design.
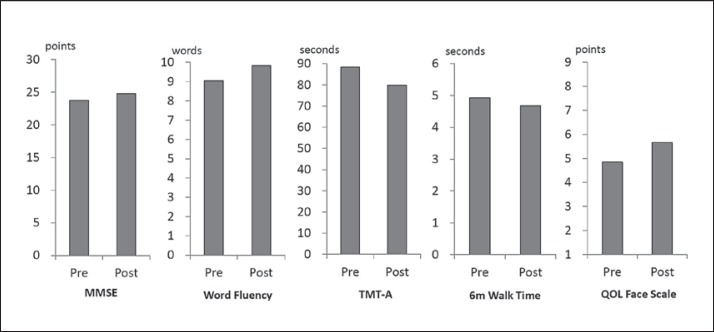
Method: A total of 127 participants aged >74 years with a CDR of 0.5 were cluster randomized into three groups for CI, PA and GRA. The intervention lasted 12 weeks and consisted of weekly group sessions and home assignments. Mini-Mental State Examination (MMSE), Trail Making Test part A (TMT-A), word fluency (WF), 6-meter walk time and Quality of Life (QOL) Face Scale scores were evaluated as primary outcomes.
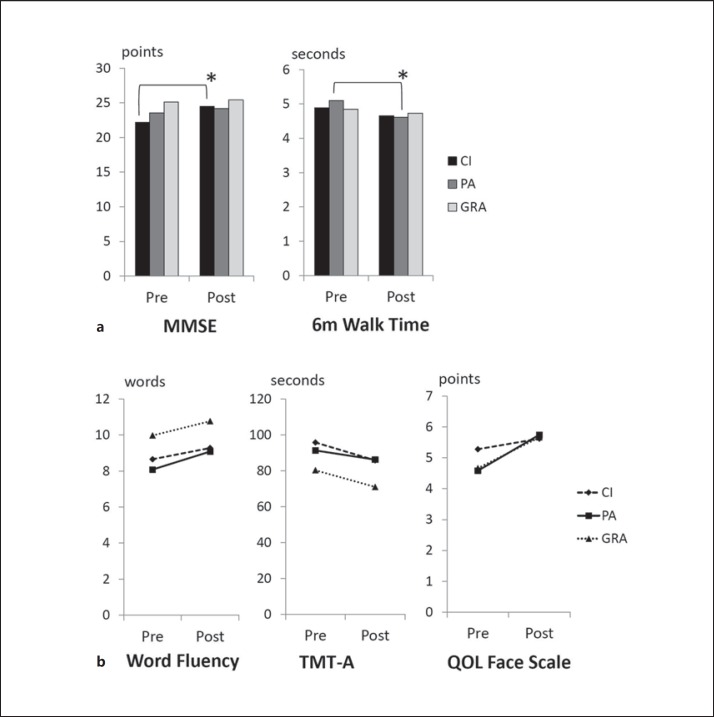
Results: Methodology-related benefits of CI and PA were found for MMSE scores and walk time, respectively. TMT-A, WF and QOL Face Scale scores improved irrespective of the methodologies used.
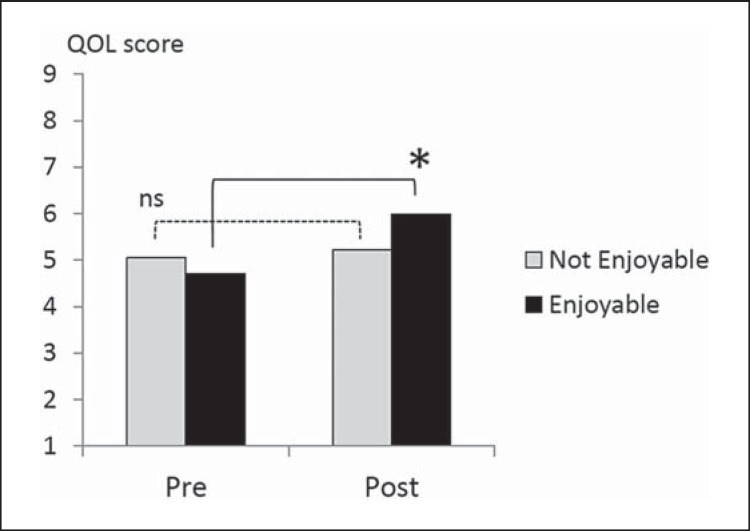
Conclusions: Our findings suggest that CI and PA may be beneficial to cognitive and physical abilities, respectively. Executive functions and QOL may improve irrespective of the intervention methodologies used.
Keywords: Clinical Dementia Rating; Nonpharmacological intervention; Old-old subjects.
Figures
References
-
- Lonie JA, Parra-Rodriguez MA, Tierney KM, Herrmann LL, Donaghey C, O'Carroll RE, Ebmeier KP. Predicting outcome in mild cognitive impairment: 4-year follow-up study. Br J Psychiatry. 2010;197:135–140. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
