

Factors Associated with the Development of Drug Resistance Mutations in HIV-1 Infected Children Failing Protease Inhibitor-Based Antiretroviral Therapy in South Africa
- PMID: 26196688
- PMCID: PMC4510388
- DOI: 10.1371/journal.pone.0133452
Factors Associated with the Development of Drug Resistance Mutations in HIV-1 Infected Children Failing Protease Inhibitor-Based Antiretroviral Therapy in South Africa
Abstract
Objective: Limited data are available from the developing world on antiretroviral drug resistance in HIV-1 infected children failing protease inhibitor-based antiretroviral therapy, especially in the context of a high tuberculosis burden. We describe the proportion of children with drug resistance mutations after failed protease inhibitor-based antiretroviral therapy as well as associated factors.
Methods: Data from children initiated on protease inhibitor-based antiretroviral therapy with subsequent virological failure referred for genotypic drug resistance testing between 2008 and 2012 were retrospectively analysed. Frequencies of drug resistance mutations were determined and associations with these mutations identified through logistic regression analysis.
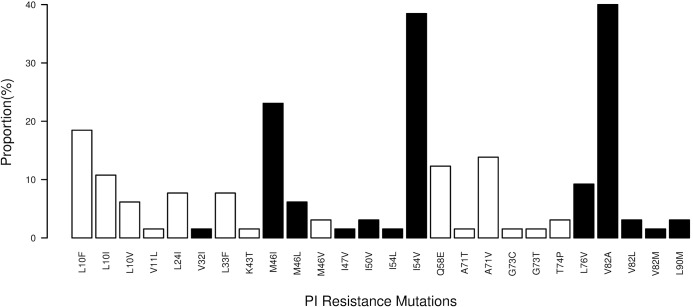
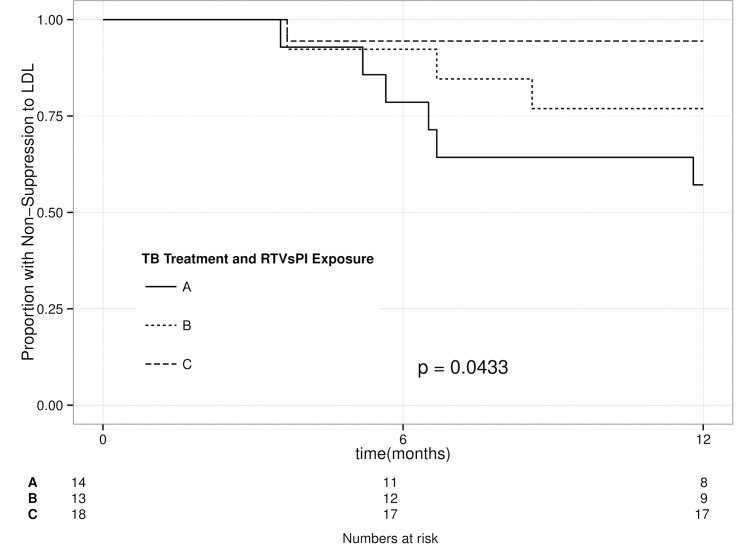
Results: The study included 65 young children (median age 16.8 months [IQR 7.8; 23.3]) with mostly advanced clinical disease (88.5% WHO stage 3 or 4 disease), severe malnutrition (median weight-for-age Z-score -2.4 [IQR -3.7;-1.5]; median height-for-age Z-score -3.1 [IQR -4.3;-2.4]), high baseline HIV viral load (median 6.04 log10, IQR 5.34;6.47) and frequent tuberculosis co-infection (66%) at antiretroviral therapy initiation. Major protease inhibitor mutations were found in 49% of children and associated with low weight-for-age and height-for-age (p = 0.039; p = 0.05); longer duration of protease inhibitor regimens and virological failure (p = 0.001; p = 0.005); unsuppressed HIV viral load at 12 months of antiretroviral therapy (p = 0.001); tuberculosis treatment at antiretroviral therapy initiation (p = 0.048) and use of ritonavir as single protease inhibitor (p = 0.038). On multivariate analysis, cumulative months on protease inhibitor regimens and use of ritonavir as single protease inhibitor remained significant (p = 0.008; p = 0.033).
Conclusion: Major protease inhibitor resistance mutations were common in this study of HIV-1-infected children, with the timing of tuberculosis treatment and subsequent protease inhibitor dosing strategy proving to be important associated factors. There is an urgent need for safe, effective, and practicable HIV/tuberculosis co-treatment in young children and the optimal timing of treatment, optimal dosing of antiretroviral therapy, and alternative tuberculosis treatment strategies should be urgently addressed.
Conflict of interest statement
Figures
Similar articles
-
Impact of lopinavir-ritonavir exposure in HIV-1 infected children and adolescents in Madrid, Spain during 2000-2014.PLoS One. 2017 Mar 28;12(3):e0173168. doi: 10.1371/journal.pone.0173168. eCollection 2017. PLoS One. 2017. PMID: 28350802 Free PMC article.
-
Mutations at codons 54 and 82 of HIV protease predict virological response of HIV-infected children on salvage lopinavir/ritonavir therapy.J Antimicrob Chemother. 2005 Dec;56(6):1081-6. doi: 10.1093/jac/dki356. Epub 2005 Sep 29. J Antimicrob Chemother. 2005. PMID: 16195257
-
Baseline HIV-1 resistance, virological outcomes, and emergent resistance in the SECOND-LINE trial: an exploratory analysis.Lancet HIV. 2015 Feb;2(2):e42-51. doi: 10.1016/S2352-3018(14)00061-7. Epub 2015 Jan 20. Lancet HIV. 2015. PMID: 26424460 Clinical Trial.
-
Study of the impact of HIV genotypic drug resistance testing on therapy efficacy.Verh K Acad Geneeskd Belg. 2001;63(5):447-73. Verh K Acad Geneeskd Belg. 2001. PMID: 11813503 Review.
-
Protease inhibitor-containing antiretroviral treatment and tuberculosis: can rifabutin fill the breach?Int J Tuberc Lung Dis. 2012 Jan;16(1):6-15. doi: 10.5588/ijtld.10.0626. Epub 2011 Aug 3. Int J Tuberc Lung Dis. 2012. PMID: 21819645 Review.
Cited by
-
Global, regional, and national prevalence of HIV-1 drug resistance in treatment-naive and treatment-experienced children and adolescents: a systematic review and meta-analysis.EClinicalMedicine. 2024 Oct 4;77:102859. doi: 10.1016/j.eclinm.2024.102859. eCollection 2024 Nov. EClinicalMedicine. 2024. PMID: 39430612 Free PMC article.
-
HIV-1 Drug Resistance and Third-Line Therapy Outcomes in Patients Failing Second-Line Therapy in Zimbabwe.Open Forum Infect Dis. 2018 Feb 2;5(2):ofy005. doi: 10.1093/ofid/ofy005. eCollection 2018 Feb. Open Forum Infect Dis. 2018. PMID: 29435471 Free PMC article.
-
Nevirapine and tuberculosis predict first-line treatment failure in HIV patients in Indonesia: Case-control study.Ann Med Surg (Lond). 2020 Oct 15;60:56-60. doi: 10.1016/j.amsu.2020.10.005. eCollection 2020 Dec. Ann Med Surg (Lond). 2020. PMID: 33133585 Free PMC article.
-
Prevalence and trends of advanced HIV disease among antiretroviral therapy-naïve and antiretroviral therapy-experienced patients in South Africa between 2010-2021: a systematic review and meta-analysis.BMC Infect Dis. 2023 Aug 22;23(1):549. doi: 10.1186/s12879-023-08521-4. BMC Infect Dis. 2023. PMID: 37608300 Free PMC article.
-
Epidemiologic and viral predictors of antiretroviral drug resistance among persons living with HIV in a large treatment program in Nigeria.AIDS Res Ther. 2020 Feb 17;17(1):7. doi: 10.1186/s12981-020-0261-z. AIDS Res Ther. 2020. PMID: 32066473 Free PMC article.
References
-
- Shearer WT, Quinn TC, LaRussa P, Lew JF, Mofenson L, Almy S, et al. Viral load and disease progression in infants infected with human immunodeficiency virus type 1. N Engl J Med 1997; 336: 1337–1342. - PubMed
-
- Abrams EJ, Weedon J, Steketee RW, Lambert G, Bamji M, Brown T, et al. Association of human immunodeficiency virus (HIV) load early in life with disease progression among HIV-infected infants. J Infect Dis 1998; 178: 101–108. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
