

A retrospective, longitudinal study estimating the association between interdialytic weight gain and cardiovascular events and death in hemodialysis patients
- PMID: 26197758
- PMCID: PMC4510887
- DOI: 10.1186/s12882-015-0110-9
A retrospective, longitudinal study estimating the association between interdialytic weight gain and cardiovascular events and death in hemodialysis patients
Abstract
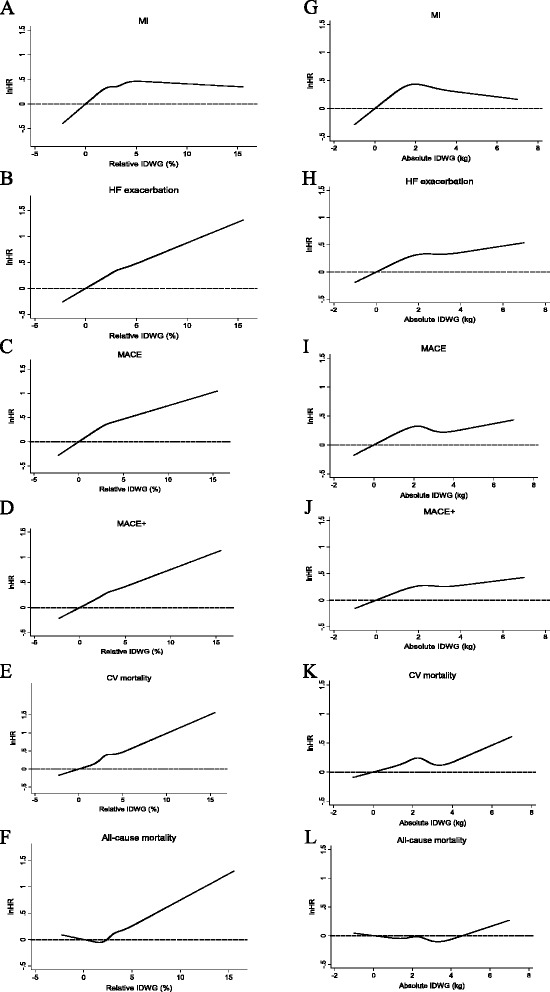
Background: Greater interdialytic weight gain (IDWG) is associated with risk of all-cause mortality and hospitalization. Dialysis patients are also at greater risk of cardiovascular (CV) events than patients without kidney disease. This retrospective study examined the potential association between IDWG and specific types of CV events.
Methods: Data were obtained from United States Renal Data System claims and the electronic health records of Medicare patients who initiated hemodialysis between 01 January 2007 and 31 December 2008 at a large dialysis organization. Absolute IDWG was defined as predialysis weight minus postdialysis weight from the prior treatment, and relative IDWG was calculated as percentage of postdialysis weight with mean values for each, calculated over dialysis days 91 to 180. Patient outcomes were considered beginning on day 181, continuing until death, discontinuation of care, censoring, or study end (31 December 2009). Outcomes included all-cause mortality, CV mortality, hospitalization for nonfatal heart failure/volume overload, hospitalization for nonfatal myocardial infarction, MACE (a composite measure of nonfatal myocardial infarction, nonfatal ischemic stroke, or CV death), and MACE+ (events comprising MACE as well as arrhythmia, nonfatal hemorrhagic stroke, or hospitalization for heart failure). Associations between IDWG and outcomes over the exposure period were estimated using proportional hazards regression and adjusted for baseline characteristics.
Results: 39,256 patients qualified for analysis. In general, associations of relative IDWG with outcomes were more potent, consistent, and monotonic than those for absolute IDWG. Relative IDWG > 3.5 % body weight was independently associated with all outcomes studied: point estimates ranged from 1.18 (myocardial infarction) to 1.26 (CV mortality) and were consistent among patients with and without diabetes, and with and without baseline heart failure. Absolute IDWG > 3 kg was associated with outcomes other than myocardial infarction: point estimates ranged from 1.11 (MACE) to 1.20 (heart failure).
Conclusions: Greater IDWG is associated with an increased risk of CV morbid events. Strategies that mitigate IDWG may improve CV health and survival among hemodialysis patients.
Figures



References
-
- United States Renal Data System . 2013 Annual Data Report: Incidence, Prevalence, Patient Characteristics, and Treatment Modalities. Bethesda: National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 2013. pp. 215–228.
-
- U S Renal Data System . 2013 Annual Data Report: Hospitalizations. Bethesda: National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 2013. pp. 237–248.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
