

Lung cancer: developments, concepts, and specific aspects of the new WHO classification
- PMID: 26197868
- PMCID: PMC11819351
- DOI: 10.1007/s00432-015-2004-4
Lung cancer: developments, concepts, and specific aspects of the new WHO classification
Abstract
Introduction: Diagnostic methods and algorithms for the diagnosis of pulmonary neoplasms have considerably changed over the recent years. Based on large-scale molecular characterization studies and the development of targeted therapies, precise morphological, immunohistochemical, and molecular pathological tumor subtyping is now of utmost importance for evidence-based treatment decisions. Changes of diagnostic concepts initially referred to biopsies and cytology specimens but are now also transferred to resection specimens.
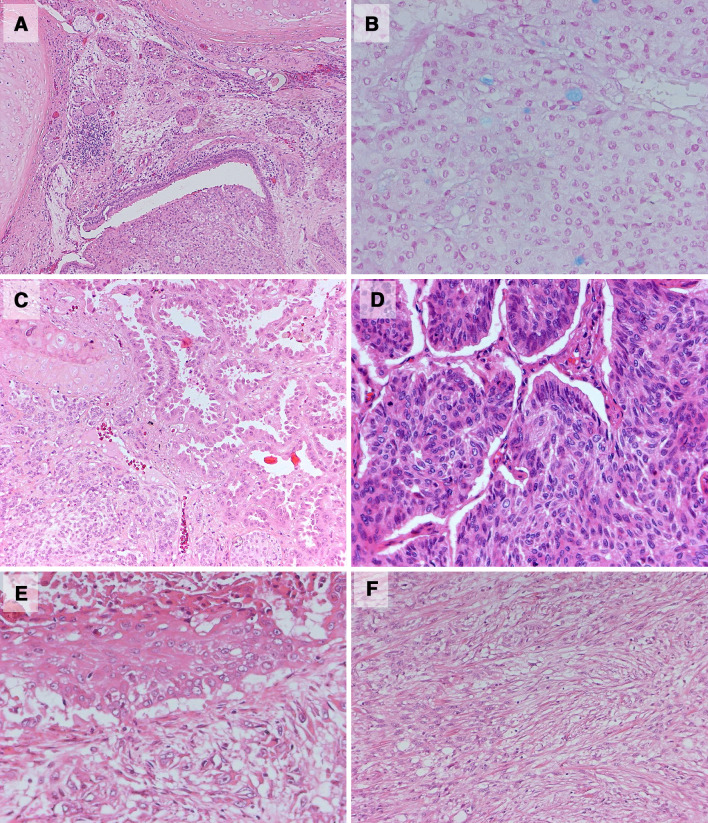
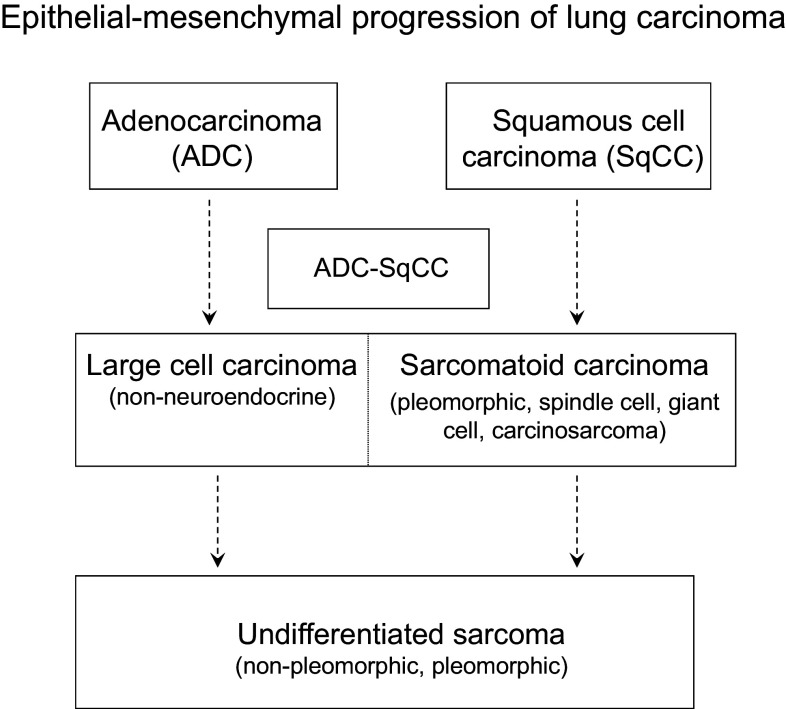
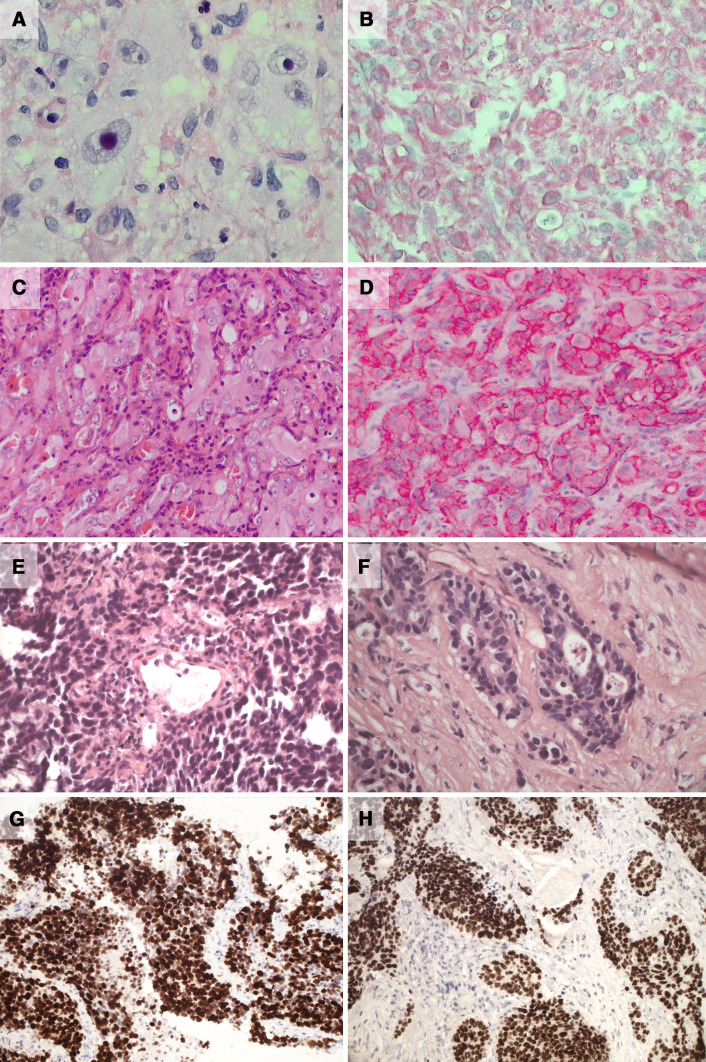
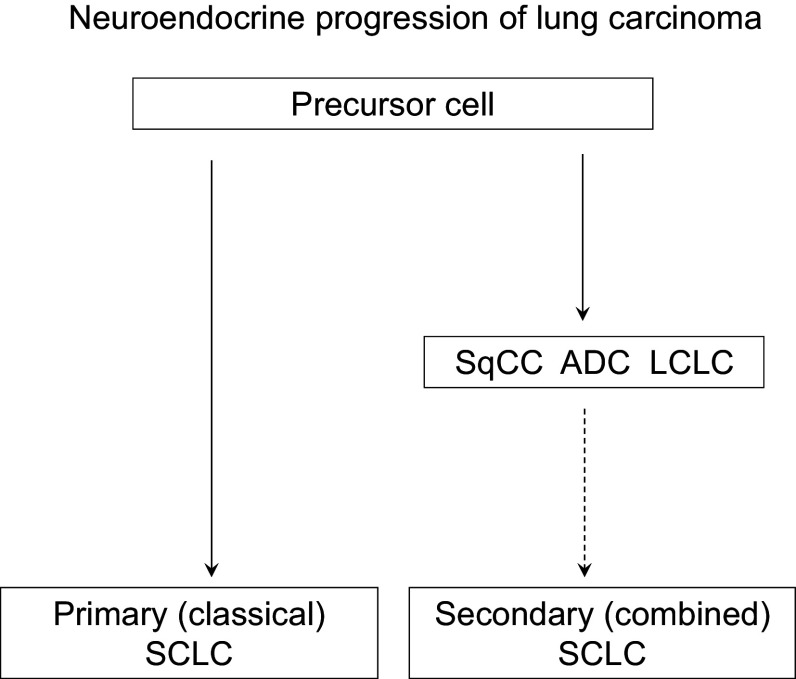
Methods: This review is focused on recent developments in morphological and immunohistochemical subtyping of pulmonary neoplasms and concepts of tumor progression. It also provides perspectives on relevant changes of diagnostic concepts within the context of the new WHO classification.
Conclusion: It becomes apparent that a three-step diagnostic concept based on morphology, immunohistochemistry, and molecular pathology is important to meet the requirements of an increasingly more complex, interdisciplinary care of lung cancer patients and to allow for reliable, clinically meaningful tumor diagnoses.
Keywords: Classification; Diagnosis; Immunohistochemistry; Lung cancer; Molecular pathology.
Conflict of interest statement
None.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
