

Assessment of Clinical Complete Response After Chemoradiation for Rectal Cancer with Digital Rectal Examination, Endoscopy, and MRI: Selection for Organ-Saving Treatment
- PMID: 26198074
- PMCID: PMC4595525
- DOI: 10.1245/s10434-015-4687-9
Assessment of Clinical Complete Response After Chemoradiation for Rectal Cancer with Digital Rectal Examination, Endoscopy, and MRI: Selection for Organ-Saving Treatment
Abstract
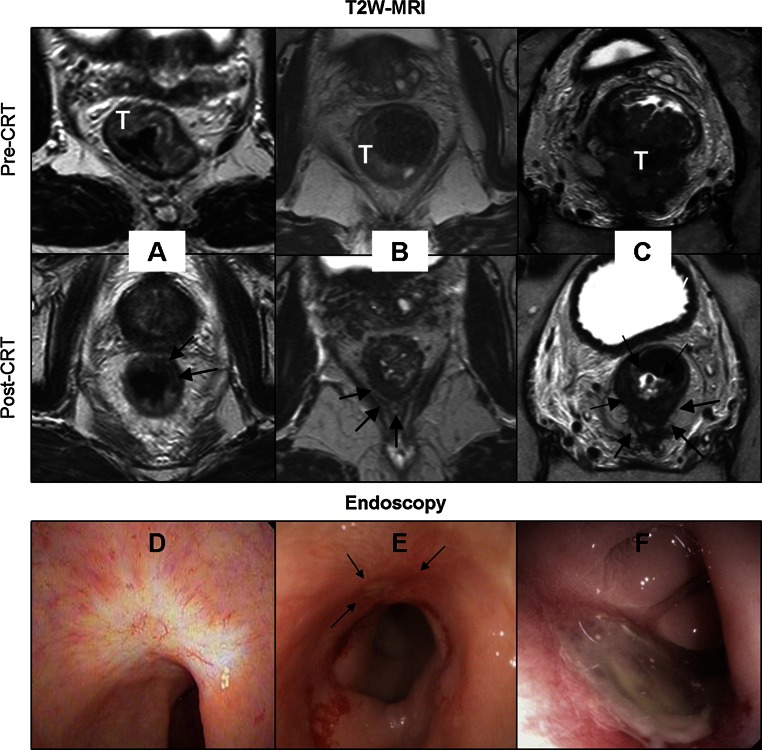
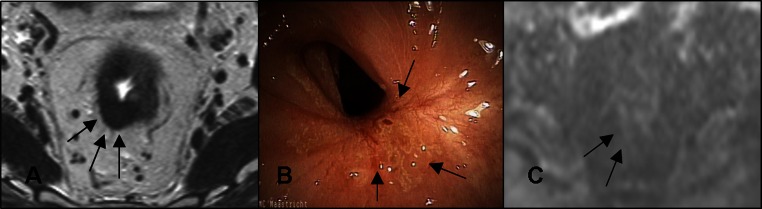
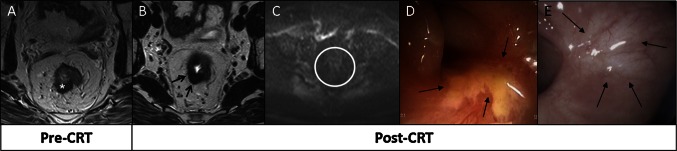
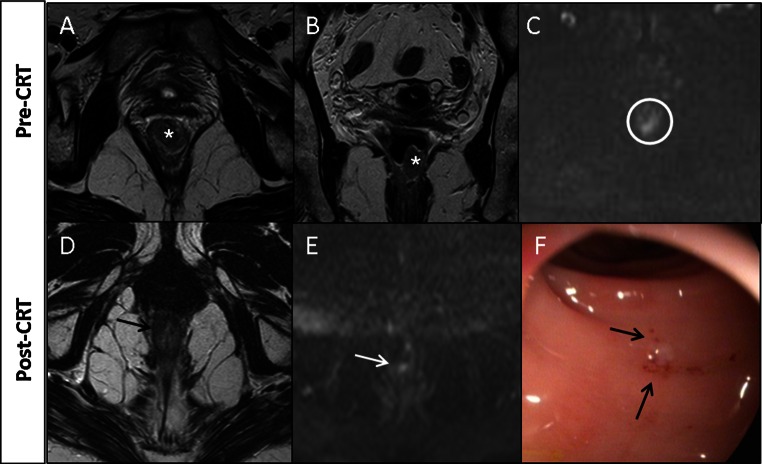
Background: The response to chemoradiotherapy (CRT) for rectal cancer can be assessed by clinical examination, consisting of digital rectal examination (DRE) and endoscopy, and by MRI. A high accuracy is required to select complete response (CR) for organ-preserving treatment. The aim of this study was to evaluate the value of clinical examination (endoscopy with or without biopsy and DRE), T2W-MRI, and diffusion-weighted MRI (DWI) for the detection of CR after CRT.
Methods: This prospective cohort study in a university hospital recruited 50 patients who underwent clinical assessment (DRE, endoscopy with or without biopsy), T2W-MRI, and DWI at 6-8 weeks after CRT. Confidence levels were used to score the likelihood of CR. The reference standard was histopathology or recurrence-free interval of >12 months in cases of wait-and-see approaches. Diagnostic performance was calculated by area under the receiver operator characteristics curve, with corresponding sensitivities and specificities. Strategies were assessed and compared by use of likelihood ratios.
Results: Seventeen (34 %) of 50 patients had a CR. Areas under the curve were 0.88 (0.78-1.00) for clinical assessment and 0.79 (0.66-0.92) for T2W-MRI and DWI. Combining the modalities led to a posttest probability for predicting a CR of 98 %. Conversely, when all modalities indicated residual tumor, 15 % of patients still experienced CR.
Conclusions: Clinical assessment after CRT is the single most accurate modality for identification of CR after CRT. Addition of MRI with DWI further improves the diagnostic performance, and the combination can be recommended as the optimal strategy for a safe and accurate selection of CR after CRT.
Figures

Comment in
-
Assessment of Clinical Complete Response After Chemoradiation for Rectal Cancer with Digital Rectal Examination, Endoscopy, and MRI.Ann Surg Oncol. 2015 Nov;22(12):3769-71. doi: 10.1245/s10434-015-4691-0. Epub 2015 Jul 1. Ann Surg Oncol. 2015. PMID: 26130453 No abstract available.
-
Watch and wait after neoadjuvant therapy for rectal cancer.Br J Surg. 2016 May;103(6):629-631. doi: 10.1002/bjs.10172. Epub 2016 Mar 17. Br J Surg. 2016. PMID: 26991060 No abstract available.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
