

Review
doi: 10.1161/CIRCIMAGING.115.003421.
Risk Stratification in Patients With Aortic Stenosis Using Novel Imaging Approaches
Affiliations
- PMID: 26198161
- PMCID: PMC4539578
- DOI: 10.1161/CIRCIMAGING.115.003421
Item in Clipboard
Review
Risk Stratification in Patients With Aortic Stenosis Using Novel Imaging Approaches
Circ Cardiovasc Imaging.
2015 Aug.
No abstract available
Keywords: aortic valve stenosis; echocardiography; endomyocardial fibrosis; magnetic resonance imaging; positron emission tomography.
Figures
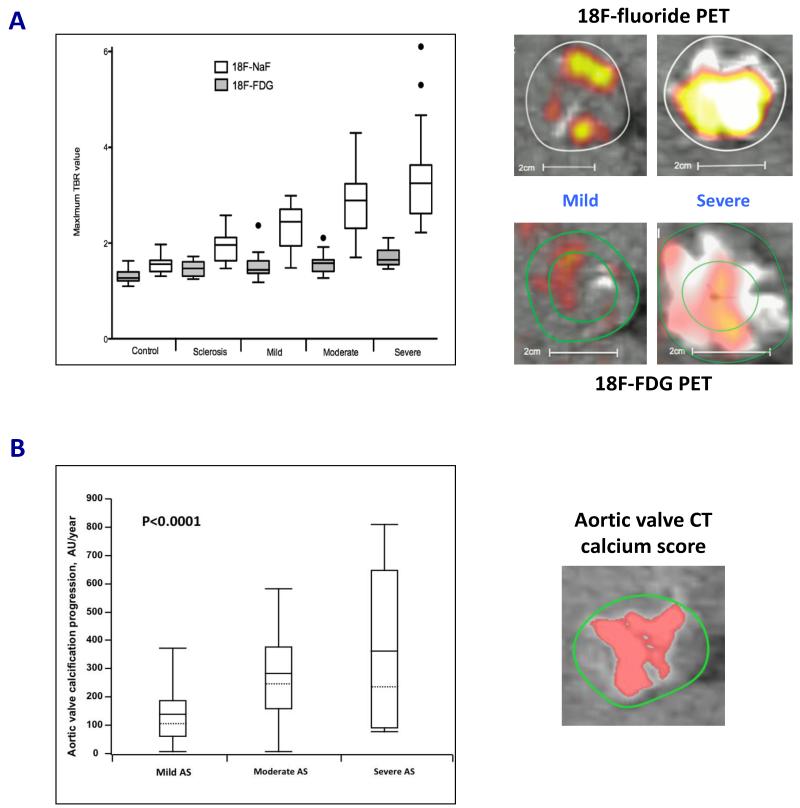
(A) 18F-Fluoride (18F-NaF; a marker of novel calcification) activity increased markedly with severity of aortic stenosis. Conversely, 18F-fluorodeoxyglucose (18F-FDG; a marker of inflammation) activity had a more modest association with aortic stenosis severity. This supports the notion that calcification rather than inflammation predominates in the valve, particularly in the later stages of the disease. Fused positron emission tomography (PET)/computed tomography (CT) scans demonstrated a significant difference in tracer activity (top right panels: 18F-NaF and bottom right panels: 18F-FDG) on co-axial views of the aortic valves in patients with mild and severe aortic stenosis. White and yellow/red areas depict calcium deposits and PET tracer activity, respectively. Results presented in box and whiskers plot (Tukey): the central box represented the interquartile range of tissue-to-background ratios (TBR) with the median indicated by the dark line. The whiskers extended to the most extreme values within the 1.5 interquartile ranges. Adapted with permission from (31). (B) Aortic valve calcification can be quantified accurately on CT (right panel). Consistent with PET data, the progression of aortic valve calcification on CT was associated with severity of aortic stenosis. Patients with severe aortic stenosis experienced increased progression of aortic valve calcification compared to those with mild or moderate disease. Results presented in box and whiskers plot: the central box represented the interquartile range, with the mean and median indicated by the dark and dotted lines, respectively. The whiskers indicated the 5th and 95th percentiles. Adapted with permission from (17).
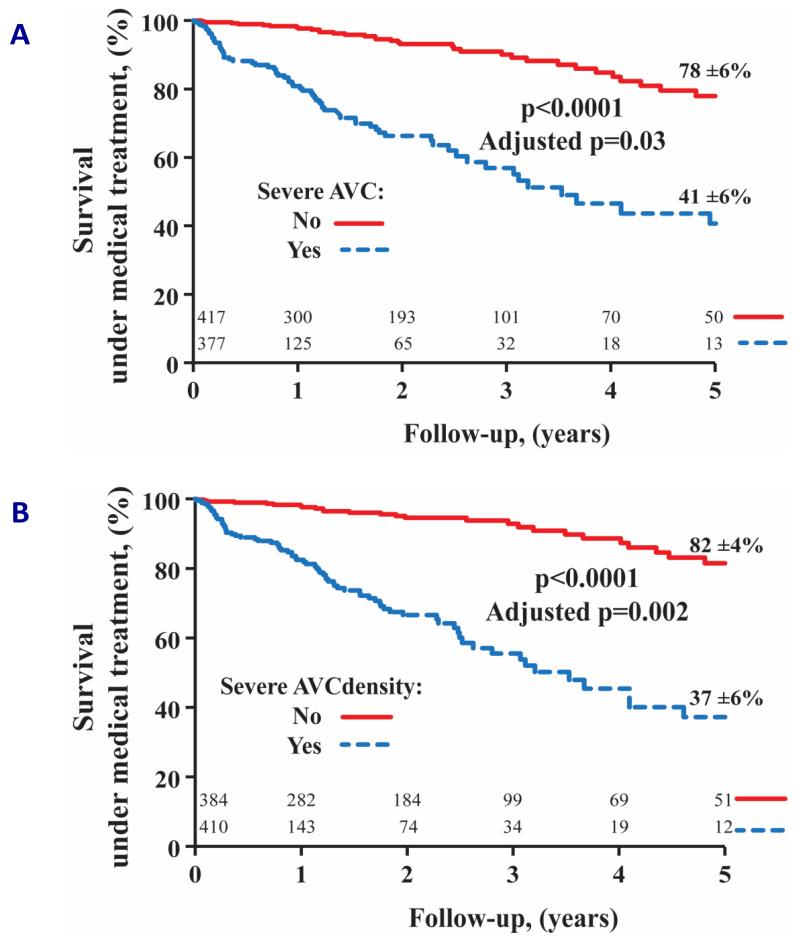
Patients with severe aortic valve calcification based on absolute aortic valve calcium score (A) or aortic valve calcification density (aortic valve calcium score indexed to aortic annular area; B) had increased all-cause mortality compared to those with non-severe aortic valve calcification. Prognostic value remained significant after adjusting for age, sex, NYHA ≥3, diabetes mellitus, coronary artery disease, indexed aortic valve area, mean pressure gradient and systolic ejection fraction. Reproduced with permission from (26).
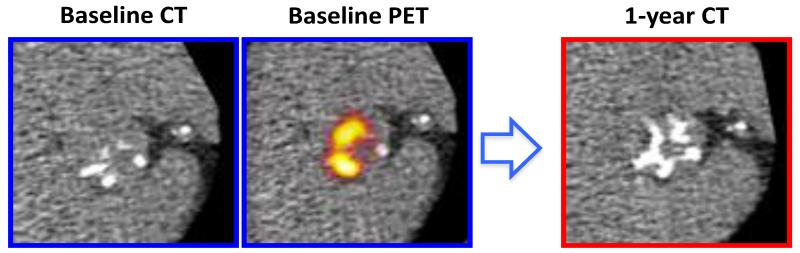
Coaxial short axis views of the aortic valve from a patient with moderate aortic stenosis demonstrated established regions of macrocalcification on baseline computed tomography (CT) scans (left blue panel). Fused 18F-fluoride positron emission tomography (PET) and CT (middle blue panel) showed increased 18F-fluoride activity in the distribution of established calcium deposits and adjacent to regions of calcification. At one year, novel calcification developed in the regions corresponding to baseline 18F-fluoride activity (right red panel).
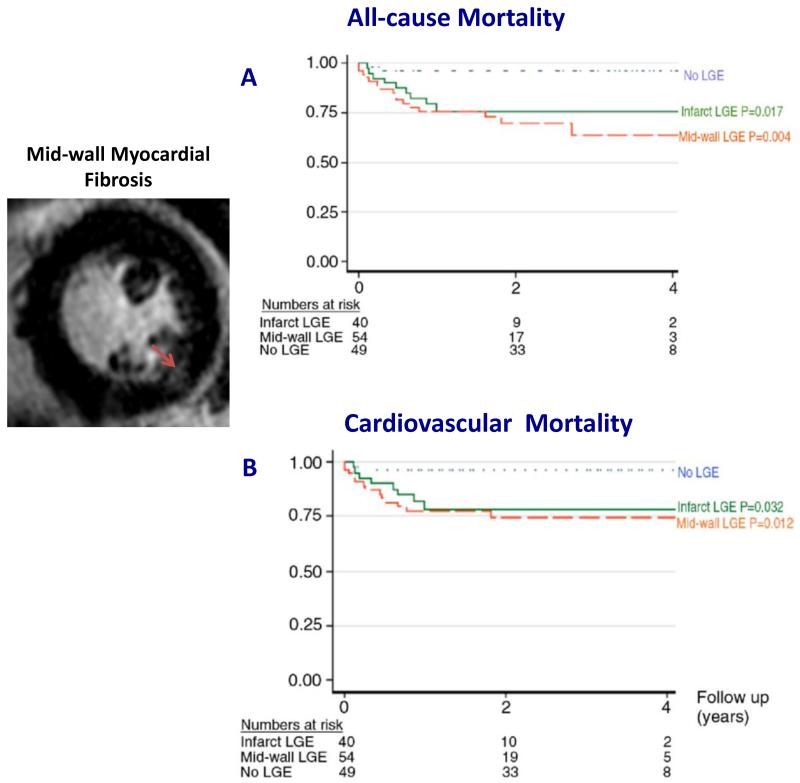
The presence of mid-wall myocardial fibrosis on cardiovascular magnetic resonance was associated with increased all-cause mortality (A) and cardiovascular mortality (B) in patients with at least moderate aortic stenosis. Adapted with permission from (42).
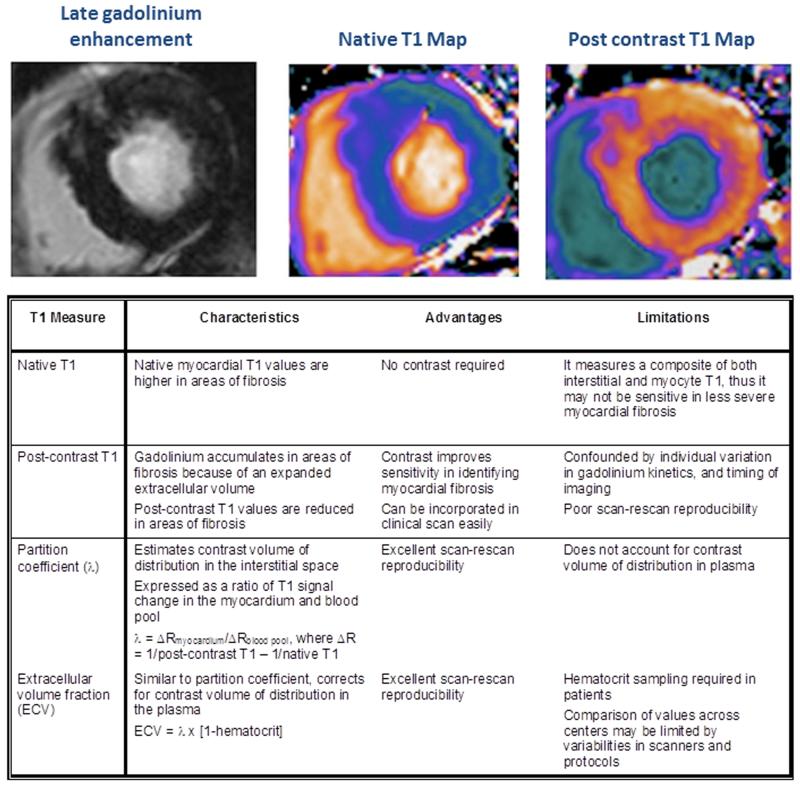
To date, there are four different myocardial T1 mapping techniques used to assess diffuse interstitial fibrosis. Each technique has its own unique merits and limitations. In aortic stenosis, extracellular volume fraction appears to be the most promising technique in assessing diffuse fibrosis. Extracellular volume fraction demonstrates excellent scan-rescan reproducibility, which is necessary when assessing change related to treatment response and disease progression.
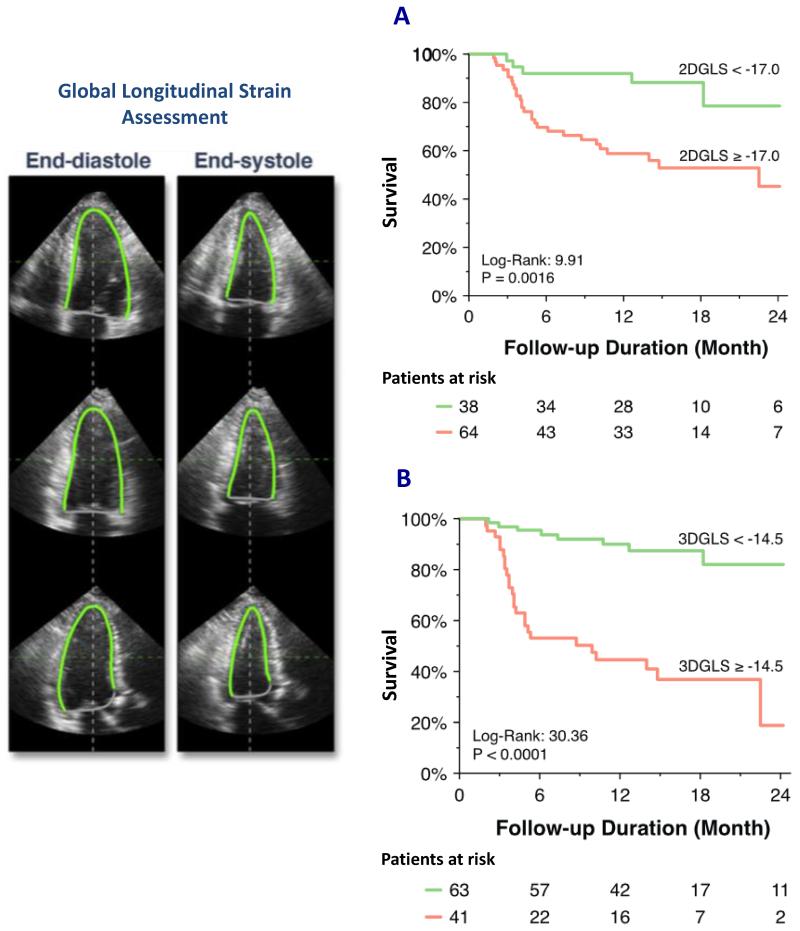
Global longitudinal strain (GLS) analysis by speckle tracking echocardiography is assessed in the 3 apical views. In this case, the endocardial borders were manually contoured and both 2D and 3D volumetric longitudinal strain can be measured. Impaired GLS assessed by either 2D or 3D speckle tracking (A and B, respectively) was associated with increased adverse cardiovascular events (cardiac death, sustained ventricular tachyarrhythmia, aortic valve replacement and hospital admission for heart failure). Reproduced with permission from (82).
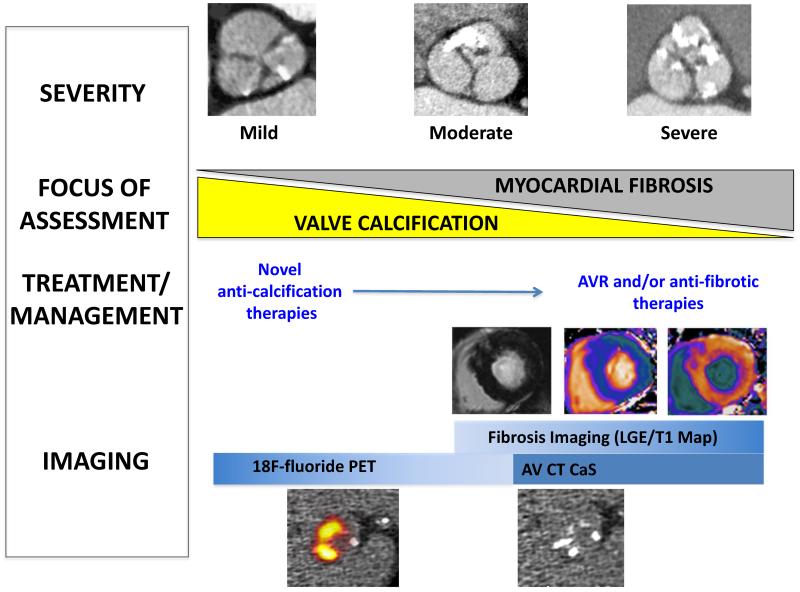
Echocardiography will remain the mainstay of imaging in the initial assessment. Aortic valve computed tomography (CT) calcium score is an alternative method in assessing aortic stenosis severity, particularly in patients with discordant echocardiographic findings. In the early stages of aortic stenosis, hybrid positron emission tomography/computed tomography (PET/CT) may complement assessment of disease progression by aortic valve CT calcium score and to monitor efficacy of novel anti-calcification therapies. In the later stages, the focus shifts to the myocardium with the aims of identifying patients with myocardial fibrosis using cardiovascular magnetic resonance, to help guide the timing of aortic valve replacement.
References
-
- Nkomo VT, Gardin JM, Skelton TN, Gottdiener JS, Scott CG, Enriquez-Sarano M. Burden of valvular heart diseases: a population-based study. Lancet. 2006;368:1005–11. - PubMed
-
- Carabello BA. Introduction to aortic stenosis. Circ Res. 2013;113:179–85. - PubMed
-
- Rajamannan NM, Evans FJ, Grande-Allen EAK, Demer LL, Heistad DD, Simmons CA, Masters KS, Mathieu P, O’Brien KD, Schoen FJ, Towler DA, Yoganathan AP, Otto CM. Calcific aortic valve disease: not simply a degenerative process: a review and agenda for Research from the National Heart and Lung and Blood Institute Aortic Stenosis Working Group Executive Summary: Calcific aortic valve disease - 2011 Update. Circulation. 2011;124:1783–91. - PMC - PubMed
-
- Ross J, Braunwald E. Aortic stenosis. Circulation. 1968;38:V61–V67. - PubMed
-
- Dweck MR, Boon NA, Newby DE. Calcific aortic stenosis: a disease of the valve and the myocardium. J Am Coll Cardiol. 2012;60:1854–63. - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
