

doi: 10.1016/j.yebeh.2015.06.028.
Epub 2015 Jul 18.
Deep hypothermia for the treatment of refractory status epilepticus
Affiliations
- PMID: 26198217
- PMCID: PMC4535418
- DOI: 10.1016/j.yebeh.2015.06.028
Item in Clipboard
Deep hypothermia for the treatment of refractory status epilepticus
Epilepsy Behav.
2015 Aug.
Abstract
In a rat model of status epilepticus (SE) induced by lithium and pilocarpine and refractory to midazolam, deep hypothermia (20 °C for 30 min) reduced EEG power over 50-fold, stopped SE within 12 min, and reduced EEG spikes by 87%. Hypothermia deserves further investigation as a treatment of last resort for refractory SE. This article is part of a Special Issue entitled "Status Epilepticus".
Keywords: EEG power; Hypothermia; Status epilepticus.
Published by Elsevier Inc.
Conflict of interest statement
None of the authors has any conflict of interest to disclose.
Figures
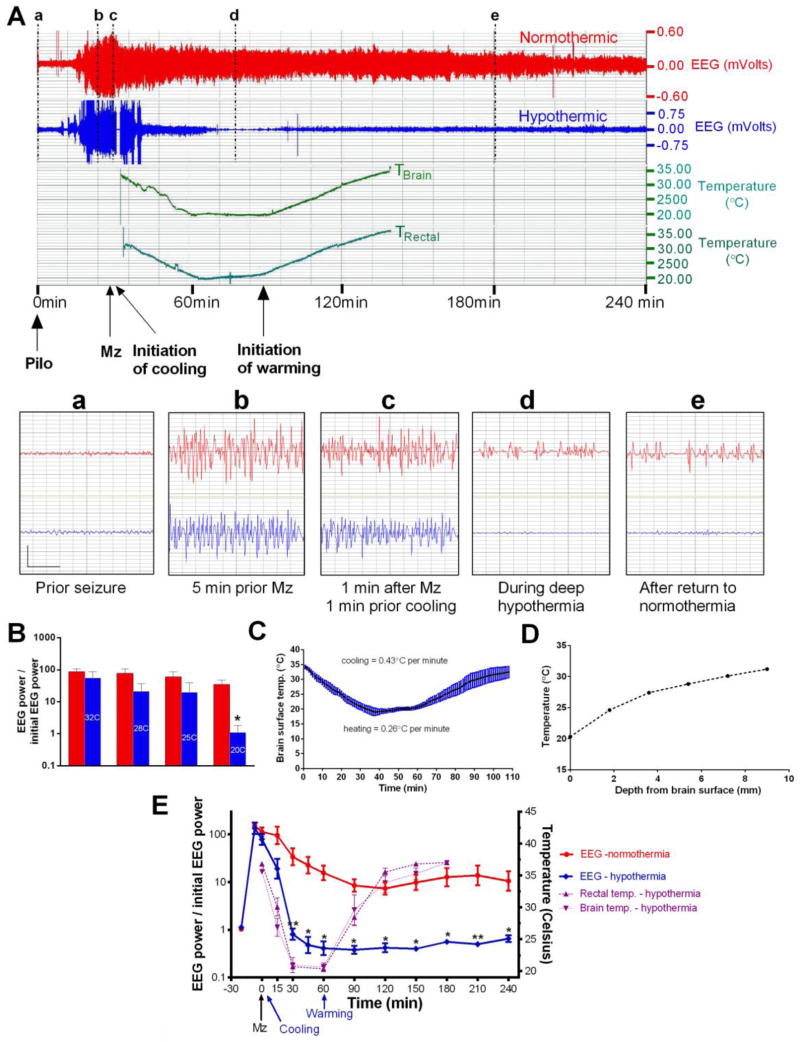
A) The upper panel shows the compressed 4-hr EEG of a normothermic (red) and a hypothermic rat (blue, 20ºC for 30 min.) with brain and rectal temperature. Both rats received midazolam 3 mg/kg ip (arrow) and cooling was initiated 2 min later. The lower panel shows the magnified 4-sec EEG traces marked by vertical lines (a–d) (vertical bar = 0.75 mV; horizontal bar = 1sec). B) Relative EEG power (EEG power/baseline EEG power) in normothermic (red bars) and hypothermic rats (blue bars, temperature in degrees Celsius) at the same time points. Relative EEG power was reduced by hypothermia in a dose-dependent fashion. The 20º C point and the slope were significantly different from normothermics (* p<0.01). C) “Brain surface” temperature during cooling and re-warming. D) Brain temperature as a function of electrode depth with the “cool cap” method. Steep temperature gradients suggest that deep structures such as the hippocampus may remain warmer than the cortical surface. E) The left y-axis of this graph shows the ratio of EEG power at each time points to initial EEG power at baseline, before pilocarpine injection. Note the logarithmic scale. Every time point beyond 30 min. showed a significant difference between normothermic and hypothermic rats (** p < 0.01; * p < 0.05). The right y-axis shows the rectal and brain temperature scales. Note that the temperature of a probe positioned at the surface of parietal cortex was close to the rectal temperature.
Similar articles
-
Effect of mild hypothermia on glutamate receptor expression after status epilepticus.Epilepsy Res. 2012 Aug;101(1-2):56-69. doi: 10.1016/j.eplepsyres.2012.03.001. Epub 2012 Apr 7. Epilepsy Res. 2012. PMID: 22487868
-
Deep hypothermia terminates status epilepticus--an experimental study.Brain Res. 2012 Mar 29;1446:119-26. doi: 10.1016/j.brainres.2012.01.022. Epub 2012 Jan 18. Brain Res. 2012. PMID: 22365745
-
Simultaneous triple therapy for the treatment of status epilepticus.Neurobiol Dis. 2017 Aug;104:41-49. doi: 10.1016/j.nbd.2017.04.019. Epub 2017 Apr 29. Neurobiol Dis. 2017. PMID: 28461248 Free PMC article.
-
Hypothermia as a treatment in status epilepticus: A narrative review.Epilepsy Behav. 2019 Dec;101(Pt B):106298. doi: 10.1016/j.yebeh.2019.04.051. Epub 2019 May 24. Epilepsy Behav. 2019. PMID: 31133509 Review.
-
Therapeutic hypothermia for status epilepticus: A report, historical perspective, and review.Clin Neurol Neurosurg. 2014 Nov;126:103-9. doi: 10.1016/j.clineuro.2014.08.032. Epub 2014 Sep 4. Clin Neurol Neurosurg. 2014. PMID: 25240131 Review.
Cited by
-
Neuroprotective effects of deep hypothermia in refractory status epilepticus.Ann Clin Transl Neurol. 2015 Nov 9;2(12):1105-15. doi: 10.1002/acn3.262. eCollection 2015 Dec. Ann Clin Transl Neurol. 2015. PMID: 26734661 Free PMC article.
-
Ketamine as adjunct to midazolam treatment following soman-induced status epilepticus reduces seizure severity, epileptogenesis, and brain pathology in plasma carboxylesterase knockout mice.Epilepsy Behav. 2020 Oct;111:107229. doi: 10.1016/j.yebeh.2020.107229. Epub 2020 Jun 20. Epilepsy Behav. 2020. PMID: 32575012 Free PMC article.
-
A New Vision for Therapeutic Hypothermia in the Era of Targeted Temperature Management: A Speculative Synthesis.Ther Hypothermia Temp Manag. 2019 Mar;9(1):13-47. doi: 10.1089/ther.2019.0001. Epub 2019 Feb 25. Ther Hypothermia Temp Manag. 2019. PMID: 30802174 Free PMC article. Review.
-
Pharmacotherapy for Pediatric Convulsive Status Epilepticus.CNS Drugs. 2020 Jan;34(1):47-63. doi: 10.1007/s40263-019-00690-8. CNS Drugs. 2020. PMID: 31879852 Free PMC article. Review.
-
Neurosteroid and benzodiazepine combination therapy reduces status epilepticus and long-term effects of whole-body sarin exposure in rats.Epilepsia Open. 2019 Jun 18;4(3):382-396. doi: 10.1002/epi4.12344. eCollection 2019 Sep. Epilepsia Open. 2019. PMID: 31440720 Free PMC article.
References
-
- Mayer SA, Claassen J, Lokin J, Mendelsohn F, Dennis LJ, Fitzsimmons BF. Refractory status epilepticus: frequency, risk factors, and impact on outcome. Arch Neurol. 2002;59:205–10. - PubMed
-
- Treiman DM, Meyers PD, Walton NY, Collins JF, Colling C, Rowan AJ, Handforth A, Faught E, Calabrese VP, Uthman BM, Ramsay RE, Mamdani MB. A comparison of four treatments for generalized convulsive status epilepticus. Veterans Affairs Status Epilepticus Cooperative Study Group. N Engl J Med. 1998;339:792–8. - PubMed
-
- Mazarati AM, Wasterlain CG. N-methyl-D-asparate receptor antagonists abolish the maintenance phase of self-sustaining status epilepticus in rat. Neurosci Lett. 1999;265:187–90. - PubMed
-
- McCullough JN, Zhang N, Reich DL, Juvonen TS, Klein JJ, Spielvogel D, Ergin MA, Griepp RB. Cerebral metabolic suppression during hypothermic circulatory arrest in humans. Ann Thorac Surg. 1999;67:1895–9. discussion 1919–21. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
