

Estimating Lead Time Gained by Optical Coherence Tomography in Detecting Glaucoma before Development of Visual Field Defects
- PMID: 26198809
- PMCID: PMC4581949
- DOI: 10.1016/j.ophtha.2015.06.015
Estimating Lead Time Gained by Optical Coherence Tomography in Detecting Glaucoma before Development of Visual Field Defects
Abstract
Purpose: To estimate the diagnostic accuracy and lead time gained by retinal nerve fiber layer (RNFL) thickness measurements from optical coherence tomography (OCT) for detecting glaucoma before the development of visual field defects.
Design: Observational cohort study.
Participants: The study group included 75 eyes of 75 patients suspected of having glaucoma. These eyes had normal standard automated perimetry (SAP) at baseline and demonstrated repeatable (3 consecutive) abnormal tests during a median follow-up of 6.3 years. A control group of 75 eyes of 75 healthy subjects matched by age and number of OCT tests during follow-up was included.
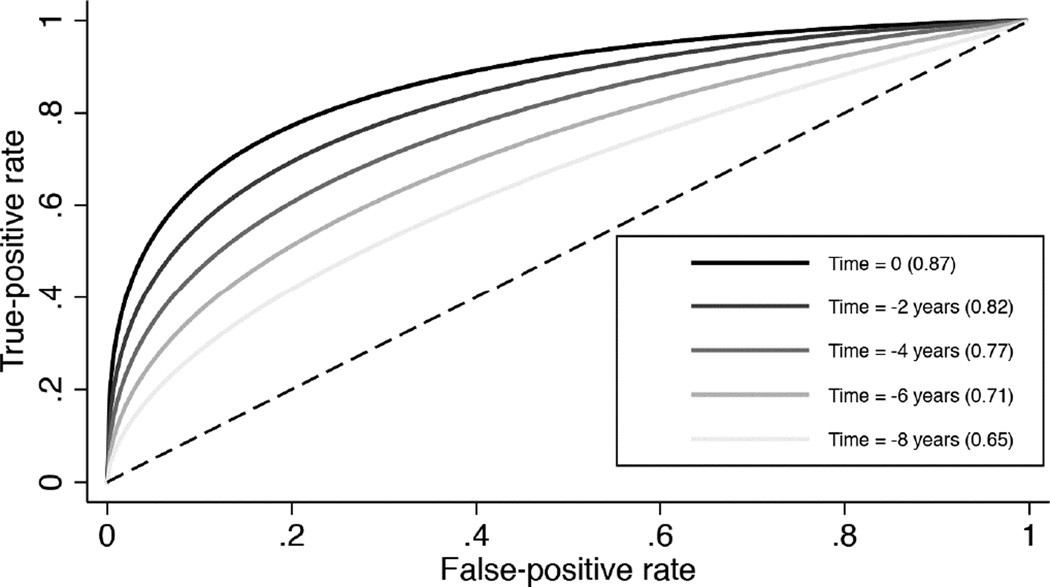
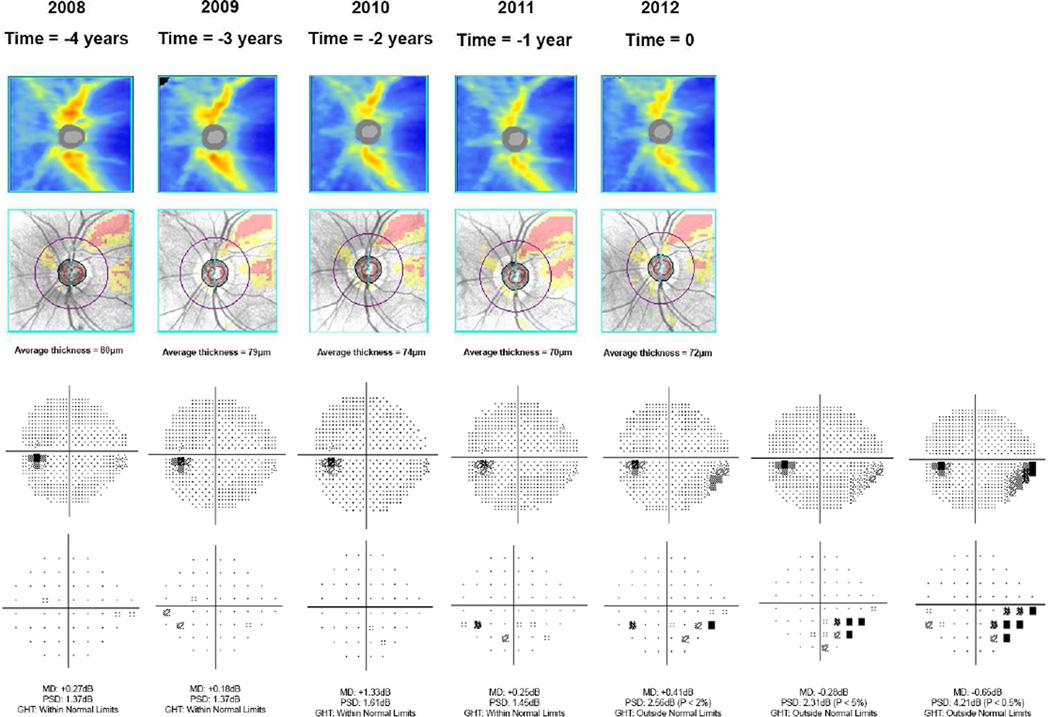
Methods: The RNFL thickness measurements were obtained at the time of development of the earliest SAP defect (time 0) and also at times -1, -2, -3, and so forth, corresponding to 1 year, 2 years, 3 years, and so forth, before the development of field loss. The OCT measurements at corresponding intervals were analyzed for controls. Time-dependent receiver operating characteristic (ROC) curves were used to evaluate diagnostic accuracy of OCT.
Main outcome measures: Areas and sensitivities of ROC curve at fixed specificities at different times before development of field loss.
Results: At the date of conversion to the earliest visual field defect (time 0), mean ± standard deviation average RNFL thickness was 75.0±9.8 μm in glaucomatous eyes and 90.6±8.0 μm for controls (P < 0.001). Significant differences were seen up to 8 years before development of visual field defects (86.3±8.2 μm vs. 91.4±7.6 μm, respectively; P = 0.021). The ROC curve areas decreased with increasing times before detection of field defects. At times 0, -4, and -8 years, ROC curve areas were 0.87, 0.77, and 0.65, respectively. At 95% specificity, up to 35% of eyes had abnormal average RNFL thickness 4 years before development of visual field loss and 19% of eyes had abnormal results 8 years before field loss.
Conclusions: Assessment of RNFL thickness with OCT was able to detect glaucomatous damage before the appearance of visual field defects on SAP. In many subjects, significantly large lead times were seen when applying OCT as an ancillary diagnostic tool.
Copyright © 2015 American Academy of Ophthalmology. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Reply.Ophthalmology. 2016 Jun;123(6):e38. doi: 10.1016/j.ophtha.2015.12.018. Ophthalmology. 2016. PMID: 27210605 No abstract available.
-
Re: Kuang et al.: Estimating lead time gained by optical coherence tomography in detecting glaucoma before development of visual field defects (Ophthalmology 2015;122:2002-9).Ophthalmology. 2016 Jun;123(6):e38. doi: 10.1016/j.ophtha.2015.10.068. Ophthalmology. 2016. PMID: 27210606 No abstract available.
-
Re: Kuang et al.: Estimating lead time gained by optical coherence topography in detecting glaucoma before development of visual field defects (Ophthalmology 2015;122:2002-9).Ophthalmology. 2016 Sep;123(9):e52-3. doi: 10.1016/j.ophtha.2015.11.036. Ophthalmology. 2016. PMID: 27549887 No abstract available.
References
-
- Gordon MO, Beiser JA, Brandt JD, et al. The Ocular Hypertension Treatment Study: baseline factors that predict the onset of primary open-angle glaucoma. Arch Ophthalmol. 2002;120:714–720. - PubMed
-
- Park SB, Sung KR, Kang SY, et al. Comparison of glaucoma diagnostic Capabilities of Cirrus HD and Stratus optical coherence tomography. Arch Ophthalmol. 2009;127:1603–1609. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
