

Prognostic robustness of serum creatinine based AKI definitions in patients with sepsis: a prospective cohort study
- PMID: 26199072
- PMCID: PMC4511260
- DOI: 10.1186/s12882-015-0107-4
Prognostic robustness of serum creatinine based AKI definitions in patients with sepsis: a prospective cohort study
Abstract
Background: It is unclear how modifications in the way to calculate serum creatinine (sCr) increase and in the cut-off value applied, influences the prognostic value of Acute Kidney Injury (AKI). We wanted to evaluate whether these modifications alter the prognostic value of AKI for prediction of mortality at 3 months, 1 and 2 years.
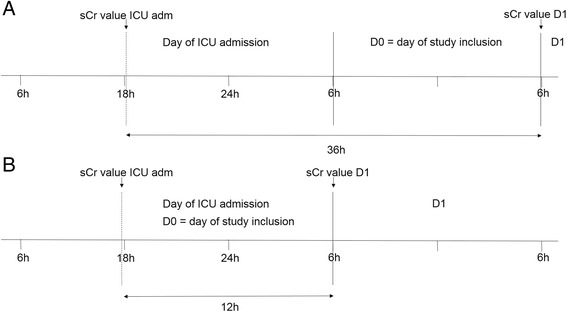
Methods: We prospectively included 195 septic patients and evaluated the prognostic value of AKI by using three different algorithms to calculate sCr increase: either as the difference between the highest value in the first 24 h after ICU admission and a pre-admission historical (ΔHIS) or an estimated (ΔEST) baseline value, or by subtracting the ICU admission value from the sCr value 24 h after ICU admission (ΔADM). Different cut-off levels of sCr increase (0.1, 0.2, 0.3, 0.4 and 0.5 mg/dl) were evaluated.
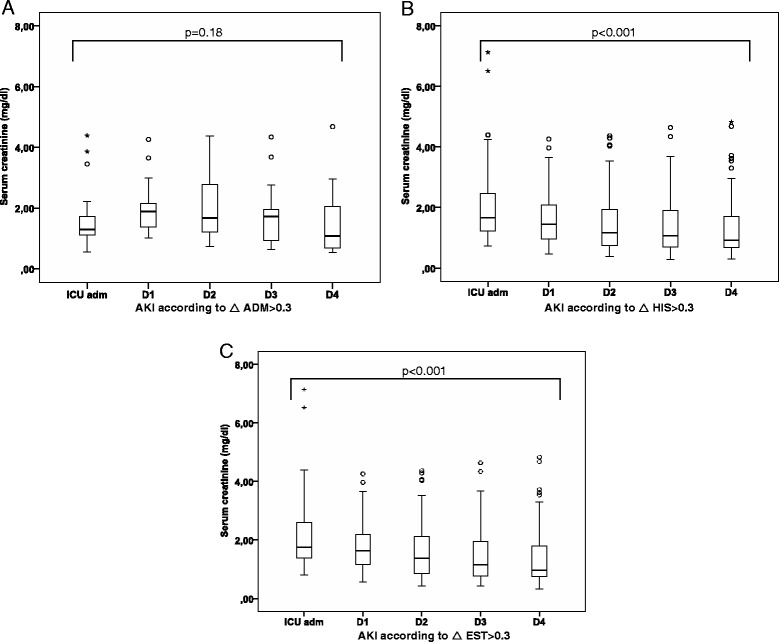
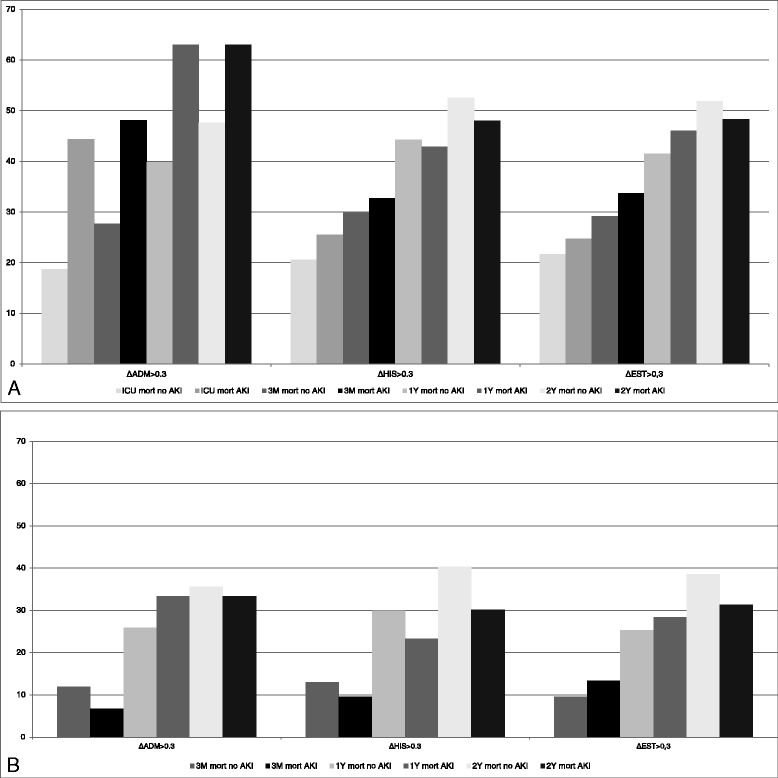
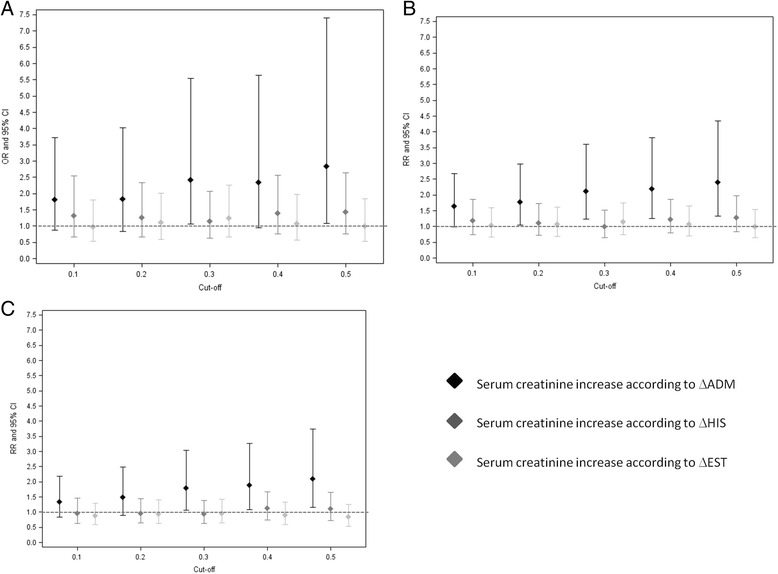
Results: Mortality at 3 months, 1 and 2 years in AKI defined as ΔADM > 0.3 mg/dl was 48.1 %, 63.0 % and 63.0 % vs 27.7 %, 39.8 % and 47.6 % in no AKI respectively (OR(95%CI): 2.42(1.06-5.54), 2.58(1.11-5.97) and 1.87(0.81-4.33); 0.3 mg/dl was the lowest cut-off value that was discriminatory. When AKI was defined as ΔHIS > 0.3 mg/dl or ΔEST > 0.3 mg/dl, there was no significant difference in mortality between AKI and no AKI.
Conclusions: The prognostic value of a 0.3 mg/dl increase in sCr, on mortality in sepsis, depends on how this sCr increase is calculated. Only if the evolution of serum creatinine over the first 24 h after ICU admission is taken into account, an association with mortality is found.
Figures
Similar articles
-
Optimum methodology for estimating baseline serum creatinine for the acute kidney injury classification.Nephrology (Carlton). 2015 Dec;20(12):881-6. doi: 10.1111/nep.12525. Nephrology (Carlton). 2015. PMID: 26032233
-
Evaluation of the Acute Kidney Injury Network criteria in hospitalized patients with cirrhosis and ascites.J Hepatol. 2013 Sep;59(3):482-9. doi: 10.1016/j.jhep.2013.03.039. Epub 2013 May 7. J Hepatol. 2013. PMID: 23665185
-
Acute kidney injury subphenotypes based on creatinine trajectory identifies patients at increased risk of death.Crit Care. 2016 Nov 17;20(1):372. doi: 10.1186/s13054-016-1546-4. Crit Care. 2016. PMID: 27852290 Free PMC article.
-
Acute kidney injury in liver cirrhosis: new definition and application.Clin Mol Hepatol. 2016 Dec;22(4):415-422. doi: 10.3350/cmh.2016.0056. Epub 2016 Dec 14. Clin Mol Hepatol. 2016. PMID: 27987536 Free PMC article. Review.
-
Creatinine-based definitions: from baseline creatinine to serum creatinine adjustment in intensive care.Crit Care. 2016 Mar 15;20:69. doi: 10.1186/s13054-016-1218-4. Crit Care. 2016. PMID: 26983854 Free PMC article. Review.
Cited by
-
Serum creatinine level and ESR values associated to clinical pathology types and prognosis of patients with renal injury caused by ANCA-associated vasculitis.Exp Ther Med. 2017 Dec;14(6):6059-6063. doi: 10.3892/etm.2017.5306. Epub 2017 Oct 16. Exp Ther Med. 2017. PMID: 29285157 Free PMC article.
-
The importance of the urinary output criterion for the detection and prognostic meaning of AKI.Sci Rep. 2021 May 27;11(1):11089. doi: 10.1038/s41598-021-90646-0. Sci Rep. 2021. PMID: 34045582 Free PMC article.
-
Clinical significance and prognosis of serum tenascin-C in patients with sepsis.BMC Anesthesiol. 2018 Nov 15;18(1):170. doi: 10.1186/s12871-018-0634-1. BMC Anesthesiol. 2018. PMID: 30442110 Free PMC article.
-
Hyperchloremia and moderate increase in serum chloride are associated with acute kidney injury in severe sepsis and septic shock patients.Crit Care. 2016 Oct 6;20(1):315. doi: 10.1186/s13054-016-1499-7. Crit Care. 2016. PMID: 27716310 Free PMC article.
-
Predictive value of the maximum serum creatinine value and growth rate in acute paraquat poisoning patients.Sci Rep. 2018 Aug 2;8(1):11587. doi: 10.1038/s41598-018-29800-0. Sci Rep. 2018. PMID: 30072769 Free PMC article. Clinical Trial.
References
-
- Lassnigg A, Schmid ER, Hiesmayr M, Falk C, Druml W, Bauer P, et al. Impact of minimal increases in serum creatinine on outcome in patients after cardiothoracic surgery: do we have to revise current definitions of acute renal failure? Crit Care Med. 2008;36:1129–1137. doi: 10.1097/CCM.0b013e318169181a. - DOI - PubMed
-
- Newsome BB, Warnock DG, McClellan WM, Herzog CA, Kiefe CI, Eggers PW, et al. Long-term risk of mortality and end-stage renal disease among the elderly after small increases in serum creatinine level during hospitalization for acute myocardial infarction. Arch Intern Med. 2008;168:609–616. doi: 10.1001/archinte.168.6.609. - DOI - PubMed
-
- Kidney disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int Suppl. 2012;2:1–138
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
