

Pulmonary CT and MRI phenotypes that help explain chronic pulmonary obstruction disease pathophysiology and outcomes
- PMID: 26199216
- PMCID: PMC5207206
- DOI: 10.1002/jmri.25010
Pulmonary CT and MRI phenotypes that help explain chronic pulmonary obstruction disease pathophysiology and outcomes
Abstract
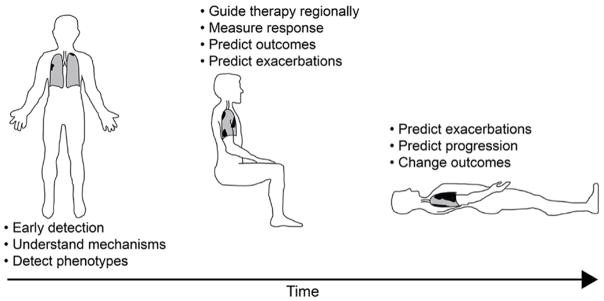
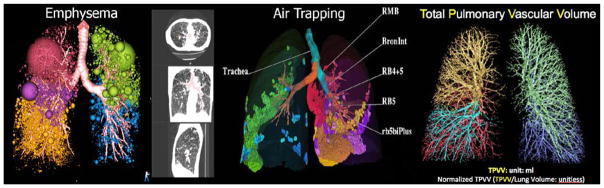
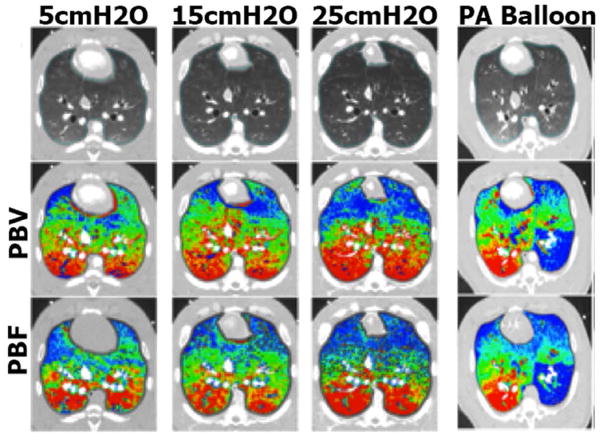
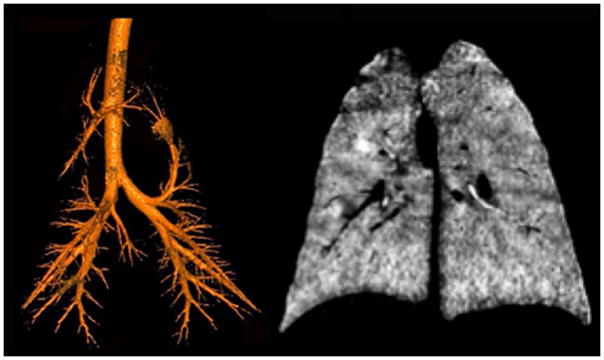
Pulmonary x-ray computed tomographic (CT) and magnetic resonance imaging (MRI) research and development has been motivated, in part, by the quest to subphenotype common chronic lung diseases such as chronic obstructive pulmonary disease (COPD). For thoracic CT and MRI, the main COPD research tools, disease biomarkers are being validated that go beyond anatomy and structure to include pulmonary functional measurements such as regional ventilation, perfusion, and inflammation. In addition, there has also been a drive to improve spatial and contrast resolution while at the same time reducing or eliminating radiation exposure. Therefore, this review focuses on our evolving understanding of patient-relevant and clinically important COPD endpoints and how current and emerging MRI and CT tools and measurements may be exploited for their identification, quantification, and utilization. Since reviews of the imaging physics of pulmonary CT and MRI and reviews of other COPD imaging methods were previously published and well-summarized, we focus on the current clinical challenges in COPD and the potential of newly emerging MR and CT imaging measurements to address them. Here we summarize MRI and CT imaging methods and their clinical translation for generating reproducible and sensitive measurements of COPD related to pulmonary ventilation and perfusion as well as parenchyma morphology. The key clinical problems in COPD provide an important framework in which pulmonary imaging needs to rapidly move in order to address the staggering burden, costs, as well as the mortality and morbidity associated with COPD.
Keywords: COPD; dual energy CT; phenotypes; pulmonary MRI; pulmonary ventilation and perfusion; quantitative CT.
© 2015 Wiley Periodicals, Inc.
Figures
References
-
- Vestbo J, Hurd SS, Agusti AG, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2013 Feb 15;187(4):347–365. - PubMed
-
- Jones PW. Health status and the spiral of decline. Copd. 2009 Feb;6(1):59–63. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
