

Advances and Prospects in Tissue-Engineered Meniscal Scaffolds for Meniscus Regeneration
- PMID: 26199629
- PMCID: PMC4496486
- DOI: 10.1155/2015/517520
Advances and Prospects in Tissue-Engineered Meniscal Scaffolds for Meniscus Regeneration
Abstract
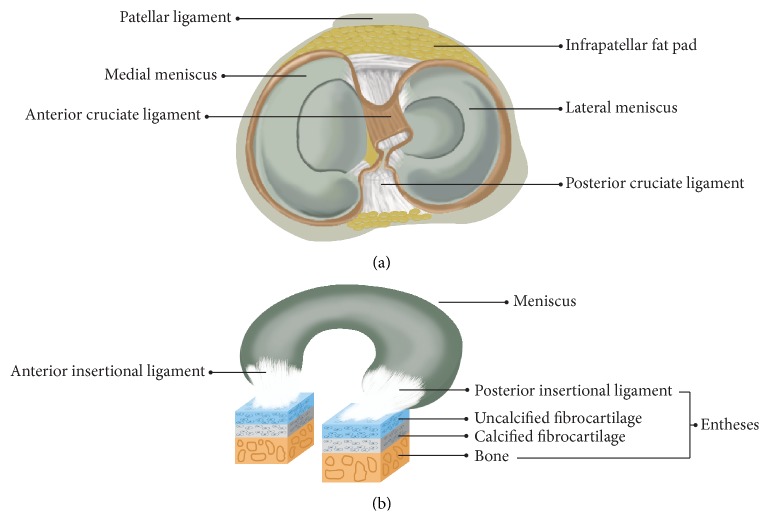
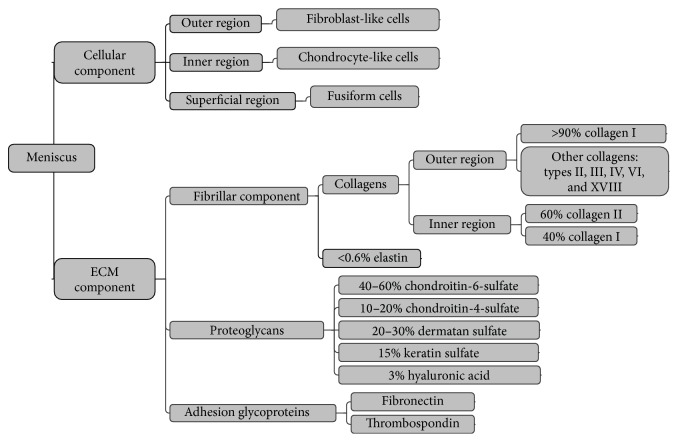
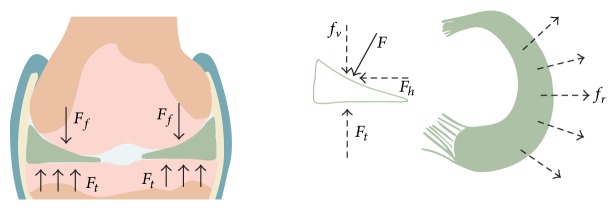
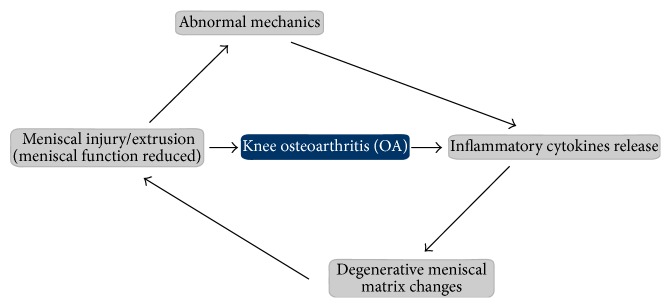
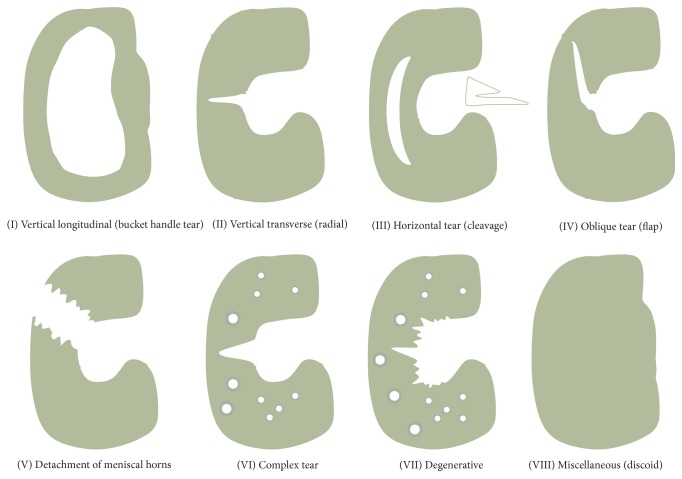
The meniscus plays a crucial role in maintaining knee joint homoeostasis. Meniscal lesions are relatively common in the knee joint and are typically categorized into various types. However, it is difficult for inner avascular meniscal lesions to self-heal. Untreated meniscal lesions lead to meniscal extrusions in the long-term and gradually trigger the development of knee osteoarthritis (OA). The relationship between meniscal lesions and knee OA is complex. Partial meniscectomy, which is the primary method to treat a meniscal injury, only relieves short-term pain; however, it does not prevent the development of knee OA. Similarly, other current therapeutic strategies have intrinsic limitations in clinical practice. Tissue engineering technology will probably address this challenge by reconstructing a meniscus possessing an integrated configuration with competent biomechanical capacity. This review describes normal structure and biomechanical characteristics of the meniscus, discusses the relationship between meniscal lesions and knee OA, and summarizes the classifications and corresponding treatment strategies for meniscal lesions to understand meniscal regeneration from physiological and pathological perspectives. Last, we present current advances in meniscal scaffolds and provide a number of prospects that will potentially benefit the development of meniscal regeneration methods.
Figures
References
-
- Scotti C., Hirschmann M. T., Antinolfi P., Martin I., Peretti G. M. Meniscus repair and regeneration: review on current methods and research potential. European Cells & Materials. 2013;26:150–170. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
