The Dens: Normal Development, Developmental Variants and Anomalies, and Traumatic Injuries
- PMID: 26199787
- PMCID: PMC4498315
- DOI: 10.4103/2156-7514.159565
The Dens: Normal Development, Developmental Variants and Anomalies, and Traumatic Injuries
Abstract
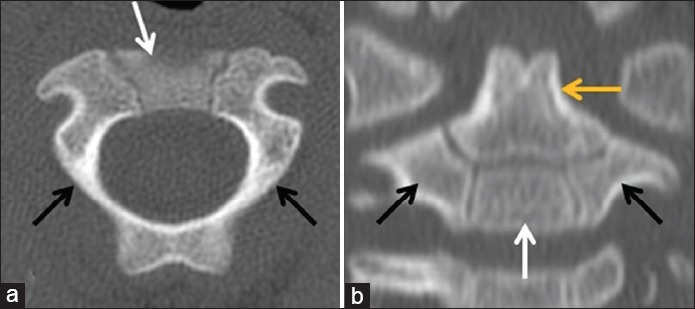
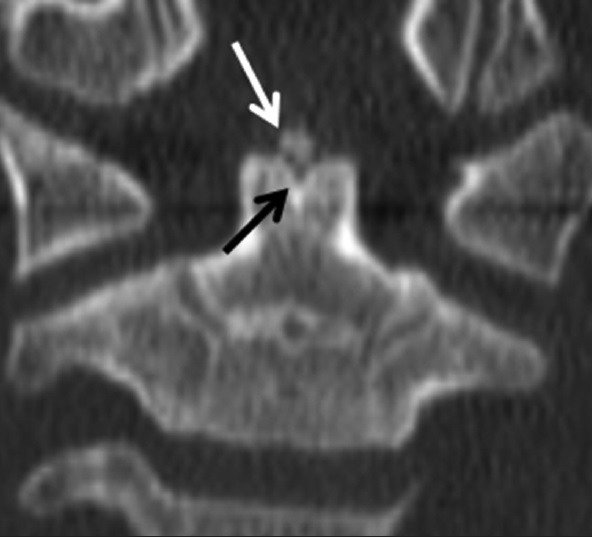
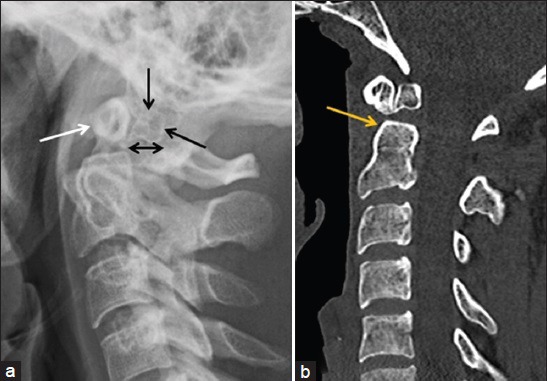
Accurate interpretation of cervical spine imagining can be challenging, especially in children and the elderly. The biomechanics of the developing pediatric spine and age-related degenerative changes predispose these patient populations to injuries centered at the craniocervical junction. In addition, congenital anomalies are common in this region, especially those associated with the axis/dens, due to its complexity in terms of development compared to other vertebral levels. The most common congenital variations of the dens include the os odontoideum and a persistent ossiculum terminale. At times, it is necessary to distinguish normal development, developmental variants, and developmental anomalies from traumatic injuries in the setting of acute traumatic injury. Key imaging features are useful to differentiate between traumatic fractures and normal or variant anatomy acutely; however, the radiologist must first have a basic understanding of the spectrum of normal developmental anatomy and its anatomic variations in order to make an accurate assessment. This review article attempts to provide the basic framework required for accurate interpretation of cervical spine imaging with a focus on the dens, specifically covering the normal development and ossification of the dens, common congenital variants and their various imaging appearances, fracture classifications, imaging appearances, and treatment options.
Keywords: Cervical vertebrae; dens axis; odontoid process; spinal anatomy; spinal injuries.
Figures


References
-
- Piatt JH, Jr, Grissom LE. Developmental anatomy of the atlas and axis in childhood by computed tomography. J Neurosurg Pediatr. 2011;8:235–43. - PubMed
-
- Lustrin ES, Karakas SP, Ortiz AO, Cinnamon J, Castillo M, Vaheesan K, et al. Pediatric cervical spine: Normal anatomy, variants, and trauma. Radiographics. 2003;23:539–60. - PubMed
-
- Ogden JA. Radiology of postnatal skeletal development. XII. The second cervical vertebra. Skeletal Radiol. 1984;12:169–77. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources