

Steroid Sex Hormones, Sex Hormone-Binding Globulin, and Diabetes Incidence in the Diabetes Prevention Program
- PMID: 26200237
- PMCID: PMC4596040
- DOI: 10.1210/jc.2015-2328
Steroid Sex Hormones, Sex Hormone-Binding Globulin, and Diabetes Incidence in the Diabetes Prevention Program
Erratum in
-
Erratum.J Clin Endocrinol Metab. 2015 Dec;100(12):4686. doi: 10.1210/jc.2015-3892. J Clin Endocrinol Metab. 2015. PMID: 26642265 Free PMC article. No abstract available.
Abstract
Context: Steroid sex hormones and SHBG may modify metabolism and diabetes risk, with implications for sex-specific diabetes risk and effects of prevention interventions.
Objective: This study aimed to evaluate the relationships of steroid sex hormones, SHBG and SHBG single-nucleotide polymorphisms (SNPs) with diabetes risk factors and with progression to diabetes in the Diabetes Prevention Program (DPP).
Design and setting: This was a secondary analysis of a multicenter randomized clinical trial involving 27 U.S. academic institutions.
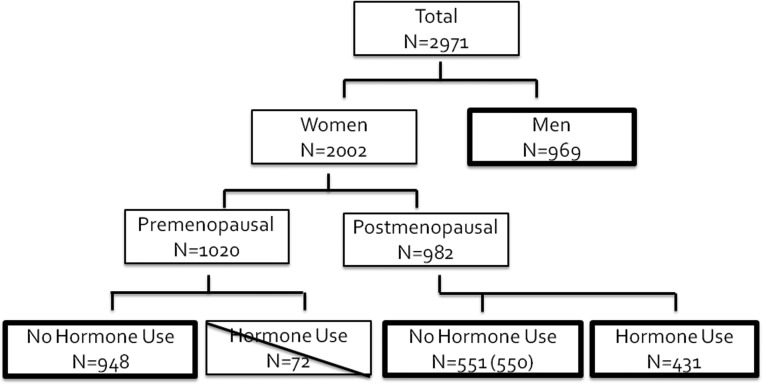
Participants: The study included 2898 DPP participants: 969 men, 948 premenopausal women not taking exogenous sex hormones, 550 postmenopausal women not taking exogenous sex hormones, and 431 postmenopausal women taking exogenous sex hormones.
Interventions: Participants were randomized to receive intensive lifestyle intervention, metformin, or placebo.
Main outcomes: Associations of steroid sex hormones, SHBG, and SHBG SNPs with glycemia and diabetes risk factors, and with incident diabetes over median 3.0 years (maximum, 5.0 y).
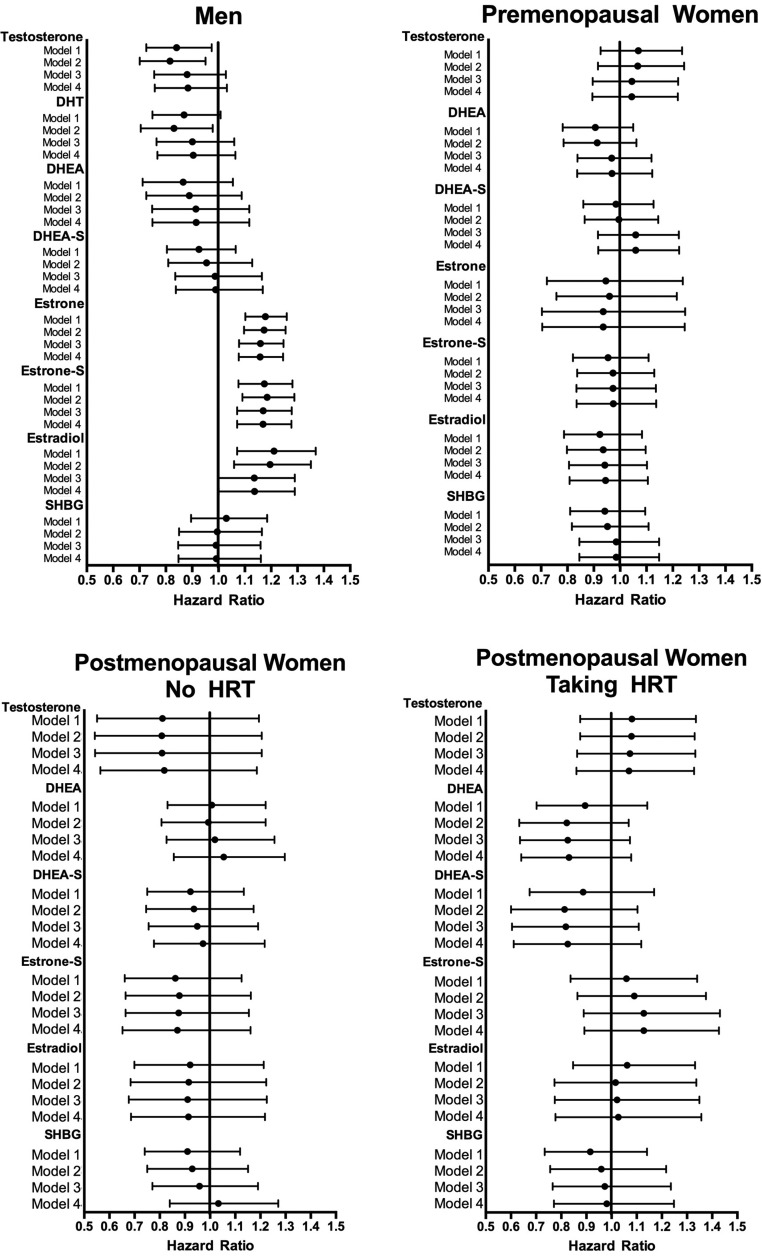
Results: T and DHT were inversely associated with fasting glucose in men, and estrone sulfate was directly associated with 2-hour post-challenge glucose in men and premenopausal women. SHBG was associated with fasting glucose in premenopausal women not taking exogenous sex hormones, and in postmenopausal women taking exogenous sex hormones, but not in the other groups. Diabetes incidence was directly associated with estrone and estradiol and inversely with T in men; the association with T was lost after adjustment for waist circumference. Sex steroids were not associated with diabetes outcomes in women. SHBG and SHBG SNPs did not predict incident diabetes in the DPP population.
Conclusions: Estrogens and T predicted diabetes risk in men but not in women. SHBG and its polymorphisms did not predict risk in men or women. Diabetes risk is more potently determined by obesity and glycemia than by sex hormones.
Trial registration: ClinicalTrials.gov NCT00004992.
Figures
Comment in
-
Letter to the Editor: "Steroid Sex Hormones, Sex Hormone-Binding Globulin, and Diabetes Incidence in the Diabetes Prevention Program" by Mather K.J., et al.J Clin Endocrinol Metab. 2015 Dec;100(12):L126-7. doi: 10.1210/jc.2015-3755. J Clin Endocrinol Metab. 2015. PMID: 26642271 No abstract available.
Similar articles
-
Circulating sex hormone binding globulin levels are modified with intensive lifestyle intervention, but their changes did not independently predict diabetes risk in the Diabetes Prevention Program.BMJ Open Diabetes Res Care. 2020 Dec;8(2):e001841. doi: 10.1136/bmjdrc-2020-001841. BMJ Open Diabetes Res Care. 2020. PMID: 33328161 Free PMC article. Clinical Trial.
-
Determinants of sex hormone-binding globulin blood concentrations in premenopausal and postmenopausal women with different estrogen status. Virgilio-Menopause-Health Group.Metabolism. 1997 Jan;46(1):5-9. doi: 10.1016/s0026-0495(97)90159-1. Metabolism. 1997. PMID: 9005961
-
The role of sex hormone-binding globulin (SHBG), testosterone, and other sex steroids, on the development of type 2 diabetes in a cohort of community-dwelling middle-aged to elderly men.Acta Diabetol. 2018 Aug;55(8):861-872. doi: 10.1007/s00592-018-1163-6. Epub 2018 May 29. Acta Diabetol. 2018. PMID: 29845345
-
Sex differences, endogenous sex-hormone hormones, sex-hormone binding globulin, and exogenous disruptors in diabetes and related metabolic outcomes.J Diabetes. 2018 Jun;10(6):428-441. doi: 10.1111/1753-0407.12517. Epub 2017 Jan 23. J Diabetes. 2018. PMID: 27990781 Review.
-
Interrelations between sex hormone-binding globulin (SHBG), plasma lipoproteins and cardiovascular risk.J Steroid Biochem Mol Biol. 1995 Jun;53(1-6):567-72. doi: 10.1016/0960-0760(95)00102-6. J Steroid Biochem Mol Biol. 1995. PMID: 7626511 Review.
Cited by
-
Sex Hormones and Measures of Kidney Function in the Diabetes Prevention Program Outcomes Study.J Clin Endocrinol Metab. 2019 Apr 1;104(4):1171-1180. doi: 10.1210/jc.2018-01495. J Clin Endocrinol Metab. 2019. PMID: 30398516 Free PMC article.
-
Diabetes and Menopause.Curr Diab Rep. 2016 Apr;16(4):20. doi: 10.1007/s11892-016-0714-x. Curr Diab Rep. 2016. PMID: 26879303 Review.
-
Sex Hormones and Diabetes in 45- to 74-year-old Men and Postmenopausal Women: The Hispanic Community Health Study.J Clin Endocrinol Metab. 2023 Jun 16;108(7):1709-1726. doi: 10.1210/clinem/dgad018. J Clin Endocrinol Metab. 2023. PMID: 36633580 Free PMC article.
-
Sex and Gender Differences in Risk, Pathophysiology and Complications of Type 2 Diabetes Mellitus.Endocr Rev. 2016 Jun;37(3):278-316. doi: 10.1210/er.2015-1137. Epub 2016 May 9. Endocr Rev. 2016. PMID: 27159875 Free PMC article. Review.
-
Association between sex steroid hormones and subsequent hyperglycemia during pregnancy.Front Endocrinol (Lausanne). 2023 Sep 8;14:1213402. doi: 10.3389/fendo.2023.1213402. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 37766683 Free PMC article.
References
-
- Ding EL, Song Y, Malik VS, Liu S. Sex differences of endogenous sex hormones and risk of type 2 diabetes: A systematic review and meta-analysis. JAMA. 2006;295(11):1288–1299. - PubMed
-
- Selvin E, Feinleib M, Zhang L, et al. Androgens and diabetes in men: Results from the Third National Health and Nutrition Examination Survey (NHANES III). Diabetes Care. 2007;30(2):234–238. - PubMed
-
- Atlantis E, Lange K, Martin S, et al. Testosterone and modifiable risk factors associated with diabetes in men. Maturitas. 2011;68(3):279–285. - PubMed
-
- Schipf S, Haring R, Friedrich N, et al. Low total testosterone is associated with increased risk of incident type 2 diabetes mellitus in men: Results from the Study of Health in Pomerania (SHIP). Aging Male. 2011;14(3):168–175. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- U01 DK048412/DK/NIDDK NIH HHS/United States
- U01 DK048375/DK/NIDDK NIH HHS/United States
- U01 DK048434/DK/NIDDK NIH HHS/United States
- U01 DK048413/DK/NIDDK NIH HHS/United States
- U01 DK048339/DK/NIDDK NIH HHS/United States
- U01 DK048468/DK/NIDDK NIH HHS/United States
- U01 DK048387/DK/NIDDK NIH HHS/United States
- U01 DK048404/DK/NIDDK NIH HHS/United States
- U01 DK048407/DK/NIDDK NIH HHS/United States
- U01 DK048437/DK/NIDDK NIH HHS/United States
- U01 DK048406/DK/NIDDK NIH HHS/United States
- R01 DK072041/DK/NIDDK NIH HHS/United States
- UL1 TR001409/TR/NCATS NIH HHS/United States
- R01 DK078907/DK/NIDDK NIH HHS/United States
- U01 DK048397/DK/NIDDK NIH HHS/United States
- U01 DK048381/DK/NIDDK NIH HHS/United States
- U01 DK048514/DK/NIDDK NIH HHS/United States
- U01 DK048485/DK/NIDDK NIH HHS/United States
- U01 DK048411/DK/NIDDK NIH HHS/United States
- U01 DK048443/DK/NIDDK NIH HHS/United States
- U01 DK048380/DK/NIDDK NIH HHS/United States
- U01 DK048400/DK/NIDDK NIH HHS/United States
- U01 DK048489/DK/NIDDK NIH HHS/United States
- U01 DK048349/DK/NIDDK NIH HHS/United States
- U01 DK048377/DK/NIDDK NIH HHS/United States
- P30 DK017047/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
