

Anesthesiologic effects of transperitoneal versus extraperitoneal approach during robot-assisted radical prostatectomy: results of a prospective randomized study
- PMID: 26200539
- PMCID: PMC4752139
- DOI: 10.1590/S1677-5538.IBJU.2014.0199
Anesthesiologic effects of transperitoneal versus extraperitoneal approach during robot-assisted radical prostatectomy: results of a prospective randomized study
Abstract
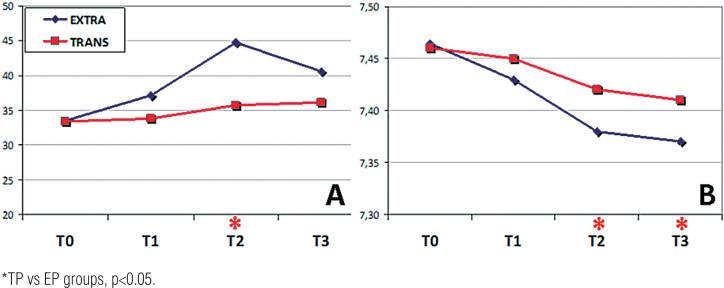
Objectives: To compare the effects of CO(2) insufflation on hemodynamics and oxygen levels and on acid-base level during Robot-Assisted Radical Prostatectomy (RARP) with transperitoneal (TP) versus extra-peritoneal (EP) accesses.
Materials and methods: Sixty-two patients were randomly assigned to TP (32) and EP (30) to RARP. Pre-operation data were collected for all patients. Hemodynamic, respiratory and blood acid-base parameters were measured at the moment of induction of anesthesia (T0), after starting CO(2) insufflation (T1), and at 60 (T2) and 120 minutes (T3) after insufflation. In all cases, the abdominal pressure was set at 15 mmHg. Complications were reported according to the Clavien-Dindo classification. Student's two-t-test, with a significance level set at p<0.05, was used to compare categorical values between groups. The Mann-Whitney U-test was used to compare the median values of two nonparametric continuous variables.
Results: The demographic characteristics of the patients in both groups were statistically comparable. Analysis of intra-operative anesthesiologic parameters showed that partial CO(2) pressure during EP was significantly higher than during TP, with a consequent decrease in arterial pH. Other parameters analysed were similar in the two groups. Postoperative complications were comparable between groups. The most important limitations of this study were the small size of the patient groups and the impossibility of maintaining standard abdominal pressure throughout the operational phases, despite attempts to regulate it.
Conclusions: This prospective randomized study demonstrates that, from the anesthesiologic viewpoint, during RARP the TP approach is preferable to EP, because of lower CO(2) reabsorption and risk of acidosis.
Figures
Similar articles
-
Transperitoneal versus extraperitoneal robot-assisted laparoscopic radical prostatectomy: A prospective single surgeon randomized comparative study.Int J Urol. 2015 Oct;22(10):916-21. doi: 10.1111/iju.12854. Epub 2015 Jul 26. Int J Urol. 2015. PMID: 26212891 Clinical Trial.
-
Transperitoneal versus extraperitoneal robotic-assisted radical prostatectomy: is one better than the other?Urology. 2006 Nov;68(5):1077-81. doi: 10.1016/j.urology.2006.07.008. Epub 2006 Nov 7. Urology. 2006. PMID: 17095060
-
[Transperitoneal versus extraperitoneal robot-assisted radical prostatectomy for localized prostate cancer].Zhonghua Nan Ke Xue. 2017 Jun;23(6):540-549. Zhonghua Nan Ke Xue. 2017. PMID: 29722948 Review. Chinese.
-
Comparison of oncological results, functional outcomes, and complications for transperitoneal versus extraperitoneal robot-assisted radical prostatectomy: a single surgeon's experience.J Endourol. 2011 May;25(5):787-92. doi: 10.1089/end.2010.0222. Epub 2010 Nov 29. J Endourol. 2011. PMID: 21114412 Clinical Trial.
-
Transperitoneal versus extraperitoneal approach to laparoscopic radical prostatectomy: an assessment of 156 cases.Urology. 2005 Feb;65(2):320-4. doi: 10.1016/j.urology.2004.09.018. Urology. 2005. PMID: 15708046 Review.
Cited by
-
Simultaneous Bilateral Video-Endoscopic Inguinal Lymphadenectomy for Penile Carcinoma: Surgical Setting, Feasibility, Safety, and Preliminary Oncological Outcomes.J Clin Med. 2023 Nov 23;12(23):7272. doi: 10.3390/jcm12237272. J Clin Med. 2023. PMID: 38068324 Free PMC article.
-
Gasless robotic perineal radical prostatectomy: An initial experience.Turk J Urol. 2018 Nov 21;45(Supp. 1):S117-S120. doi: 10.5152/tud.2018.48085. Print 2019 Nov. Turk J Urol. 2018. PMID: 30475698 Free PMC article.
-
International multicenter observational study on assessment of ventilatory management during general anaesthesia for robotic surgery and its effects on postoperative pulmonary complication (AVATaR): study protocol and statistical analysis plan.BMJ Open. 2018 Aug 23;8(8):e021643. doi: 10.1136/bmjopen-2018-021643. BMJ Open. 2018. PMID: 30139899 Free PMC article.
-
Extraperitoneal Robot-Assisted Laparoscopic Radical Prostatectomy in Continuous Spinal Anesthesia: A New Approach to an Established Technique.Medicina (Kaunas). 2024 Dec 1;60(12):1973. doi: 10.3390/medicina60121973. Medicina (Kaunas). 2024. PMID: 39768853 Free PMC article.
-
Individualized PEEP without Recruitment Maneuvers Improves Intraoperative Oxygenation: A Randomized Controlled Study.Bioengineering (Basel). 2023 Oct 9;10(10):1172. doi: 10.3390/bioengineering10101172. Bioengineering (Basel). 2023. PMID: 37892902 Free PMC article.
References
-
- Ficarra V, Novara G, Artibani W, Cestari A, Galfano A, Graefen M, et al. Retropubic, laparoscopic, and robot-assisted radical prostatectomy: a systematic review and cumulative analysis of comparative studies. Eur Urol. 2009;55:1037–1063. - PubMed
-
- Meininger D, Byhahn C, Wolfram M, Mierdl S, Kessler P, Westphal K. Prolonged intraperitoneal versus extraperitoneal insufflation of carbon dioxide in patients undergoing totally endoscopic robot-assisted radical prostatectomy. Surg Endosc. 2004;18:829–833. - PubMed
-
- Youssef MA, Al Mulhim A. Physiologic effects of pneumoperitoneum in adults with sickle cell disease undergoing laparoscopic cholecystectomy (a case control study) Surg Endosc. 2008;22:1513–1518. - PubMed
-
- Kanwer DB, Kaman L, Nedounsejiane M, Medhi B, Verma GR, Bala I. Comparative study of low pressure versus standard pressure pneumoperitoneum in laparoscopic cholecystectomy-a randomised controlled trial. Trop Gastroenterol. 2009;30:171–174. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical