

Lower Extremity Proximal Muscle Function and Dyspnea in Older Persons
- PMID: 26200804
- PMCID: PMC5283074
- DOI: 10.1111/jgs.13529
Lower Extremity Proximal Muscle Function and Dyspnea in Older Persons
Abstract
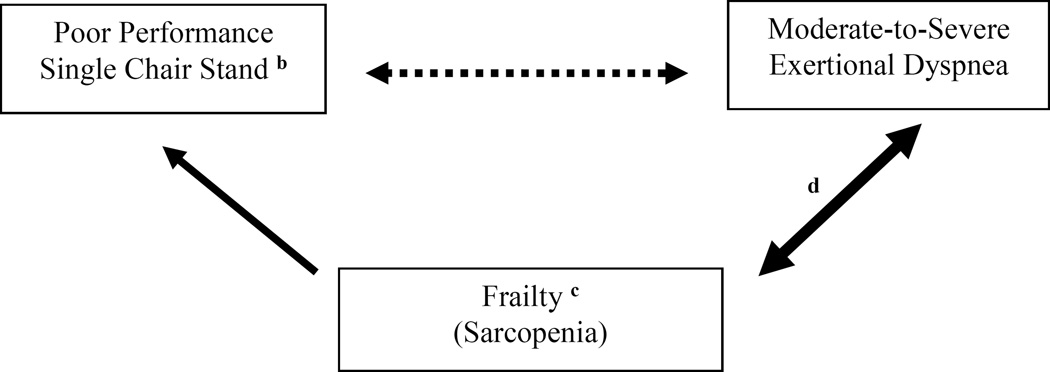
Objectives: To evaluate the association between performance on a single chair stand and moderate to severe exertional dyspnea.
Design: Cross-sectional.
Setting: Cardiovascular Health Study.
Participants: Community-dwelling individuals aged 65 and older (N = 4,413; mean age 72.6; female, n = 2,518 (57.1%); nonwhite, n = 199 (4.5%); obese, n = 788 (17.9%); history of smoking, n = 2,410 (54.6%)).
Measurements: Performance on single chair stand (poor (unable to rise without arm use) vs normal (able to rise without arm use)), moderate to severe exertional dyspnea (American Thoracic Society grade ≥2), age, sex, ethnicity, obesity, smoking, frailty status (Fried-defined nonfrail, prefrail, frail), high cardiopulmonary risk (composite of cardiopulmonary diseases and diabetes mellitus), spirometric impairment, arthritis, depression, stroke, and kidney disease.
Results: Poor performance on the single chair stand was established in 369 (8.4%) and moderate to severe exertional dyspnea in 773 (17.5%). Prefrail status was established in 2,210 (50.1%), frail status in 360 (8.2%), arthritis in 2,241 (51.4%), high cardiopulmonary risk in 2,469 (55.9%), spirometric impairment in 1,076 (24.4%), kidney disease in 111 (2.5%), depression in 107 (2.4%), and stroke in 93 (2.1%). In multivariable regression models, poor performance on the single chair stand was associated with moderate to severe exertional dyspnea (unadjusted odds ratio (OR) = 3.48, 95% confidence interval (CI) = 2.78-4.36; adjusted OR = 1.85, 95% CI = 1.41-2.41).
Conclusion: Poor performance on a single chair stand was associated with an adjusted 85% greater likelihood of moderate to severe exertional dyspnea than normal performance. These results suggest that reduced proximal muscle function of the lower extremities is associated with moderate to severe exertional dyspnea, even after adjusting for multiple confounders.
Keywords: chair stand; dyspnea; spirometry.
© 2015, Copyright the Authors Journal compilation © 2015, The American Geriatrics Society.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
References
-
- Kroenke K, Arrington ME, Mangelsdorff AD. The prevalence of symptoms in medical outpatients and the adequacy of therapy. Arch Intern Med. 1990;150:1685–1689. - PubMed
-
- Enright P, Kronmal RA, Higgins MW, et al. Prevalence and correlates of respiratory symptoms and disease in the elderly. Chest. 1994;106:827–834. - PubMed
-
- Huijnen B, van der Horst F, van Amelsvoort L, et al. Dyspnea in elderly family practice patients. Occurrence, severity, quality of life and mortality over an 8-year period. Family Practice. 2006;23:34–39. - PubMed
-
- Tessier JF, Nejjari C, Letteneur L, et al. Dyspnea and 8-year mortality among elderly men and women: the PAQUID cohort study. Eur J Epidemiol. 2001;17:223–229. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
