

Testosterone deficiency increases hospital readmission and mortality rates in male patients with heart failure
- PMID: 26200897
- PMCID: PMC4592174
- DOI: 10.5935/abc.20150078
Testosterone deficiency increases hospital readmission and mortality rates in male patients with heart failure
Abstract
Background: Testosterone deficiency in patients with heart failure (HF) is associated with decreased exercise capacity and mortality; however, its impact on hospital readmission rate is uncertain. Furthermore, the relationship between testosterone deficiency and sympathetic activation is unknown.
Objective: We investigated the role of testosterone level on hospital readmission and mortality rates as well as sympathetic nerve activity in patients with HF.
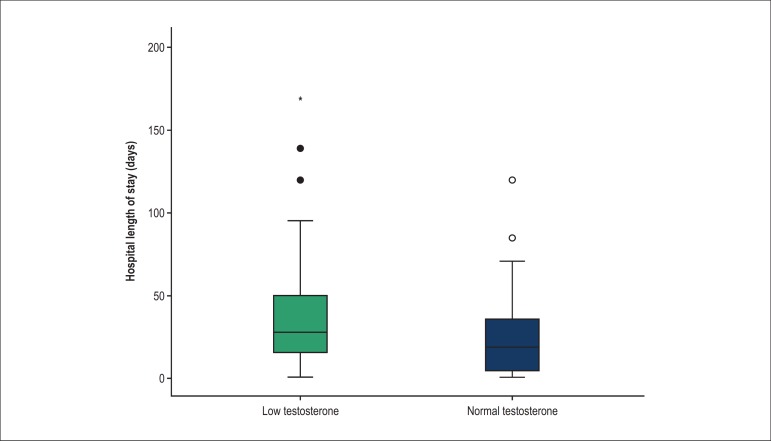
Methods: Total testosterone (TT) and free testosterone (FT) were measured in 110 hospitalized male patients with a left ventricular ejection fraction < 45% and New York Heart Association classification IV. The patients were placed into low testosterone (LT; n = 66) and normal testosterone (NT; n = 44) groups. Hypogonadism was defined as TT < 300 ng/dL and FT < 131 pmol/L. Muscle sympathetic nerve activity (MSNA) was recorded by microneurography in a subpopulation of 27 patients.
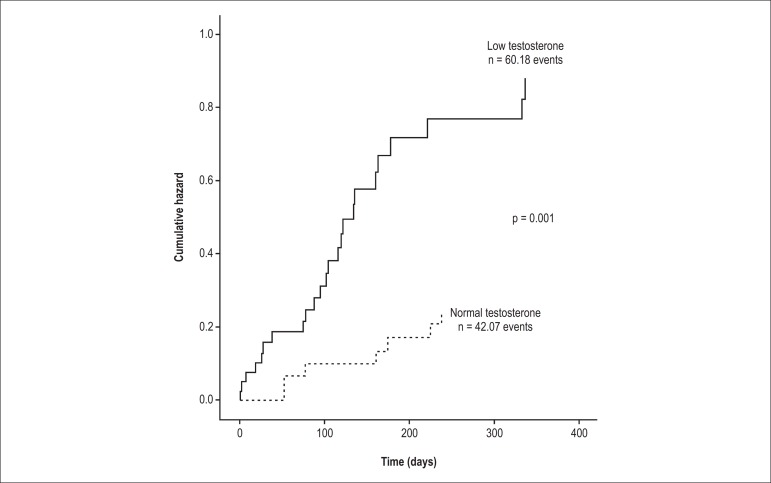
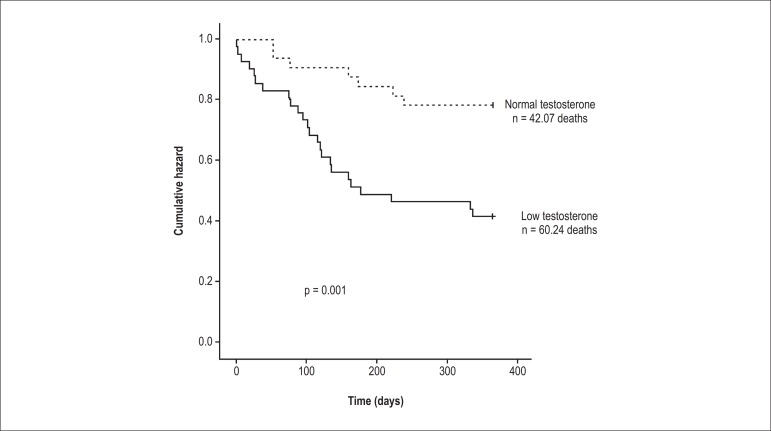
Results: Length of hospital stay was longer in the LT group compared to in the NT group (37 ± 4 vs. 25 ± 4 days; p = 0.008). Similarly, the cumulative hazard of readmission within 1 year was greater in the LT group compared to in the NT group (44% vs. 22%, p = 0.001). In the single-predictor analysis, TT (hazard ratio [HR], 2.77; 95% confidence interval [CI], 1.58-4.85; p = 0.02) predicted hospital readmission within 90 days. In addition, TT (HR, 4.65; 95% CI, 2.67-8.10; p = 0.009) and readmission within 90 days (HR, 3.27; 95% CI, 1.23-8.69; p = 0.02) predicted increased mortality. Neurohumoral activation, as estimated by MSNA, was significantly higher in the LT group compared to in the NT group (65 ± 3 vs. 51 ± 4 bursts/100 heart beats; p < 0.001).
Conclusion: These results support the concept that LT is an independent risk factor for hospital readmission within 90 days and increased mortality in patients with HF. Furthermore, increased MSNA was observed in patients with LT.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
Similar articles
-
Associations Between Short or Long Length of Stay and 30-Day Readmission and Mortality in Hospitalized Patients With Heart Failure.JACC Heart Fail. 2017 Aug;5(8):578-588. doi: 10.1016/j.jchf.2017.03.012. Epub 2017 May 10. JACC Heart Fail. 2017. PMID: 28501521
-
Relation of Acute Heart Failure Hospital Length of Stay to Subsequent Readmission and All-Cause Mortality.Am J Cardiol. 2015 Aug 1;116(3):400-5. doi: 10.1016/j.amjcard.2015.04.052. Epub 2015 May 9. Am J Cardiol. 2015. PMID: 26037295
-
Associations between aldosterone antagonist therapy and risks of mortality and readmission among patients with heart failure and reduced ejection fraction.JAMA. 2012 Nov 28;308(20):2097-107. doi: 10.1001/jama.2012.14795. JAMA. 2012. PMID: 23188026
-
Effect of Exercise Training and Testosterone Replacement on Skeletal Muscle Wasting in Patients With Heart Failure With Testosterone Deficiency.Mayo Clin Proc. 2016 May;91(5):575-86. doi: 10.1016/j.mayocp.2016.02.014. Epub 2016 Mar 31. Mayo Clin Proc. 2016. PMID: 27040087 Clinical Trial.
-
Outcomes of heart failure with preserved ejection fraction in a Southeast Asian cohort.J Cardiovasc Med (Hagerstown). 2015 Sep;16(9):583-90. doi: 10.2459/JCM.0000000000000100. J Cardiovasc Med (Hagerstown). 2015. PMID: 25022929 Review.
Cited by
-
Final Results of a Randomized, Placebo-Controlled, Two-Arm, Parallel Clinical Trial of Proxalutamide for Hospitalized COVID-19 Patients: A Multiregional, Joint Analysis of the Proxa-Rescue AndroCoV Trial.Cureus. 2021 Dec 25;13(12):e20691. doi: 10.7759/cureus.20691. eCollection 2021 Dec. Cureus. 2021. PMID: 34976549 Free PMC article.
-
Testosterone Replacement Therapy and Mortality in Older Men.Drug Saf. 2016 Feb;39(2):117-30. doi: 10.1007/s40264-015-0348-y. Drug Saf. 2016. PMID: 26482385 Review.
-
Effect of High Testosterone Levels on Endothelial Function in Aorta and Erectile Function in Rats.Sex Med. 2022 Oct;10(5):100550. doi: 10.1016/j.esxm.2022.100550. Epub 2022 Aug 5. Sex Med. 2022. PMID: 35939869 Free PMC article.
-
A 3-year observation of testosterone deficiency in Chinese patients with chronic heart failure.Oncotarget. 2017 Aug 2;8(45):79835-79842. doi: 10.18632/oncotarget.19816. eCollection 2017 Oct 3. Oncotarget. 2017. PMID: 29108365 Free PMC article.
-
Testosterone antagonizes paraquat-induced cardiomyocyte senescence via the mIGF-1/SIRT1 signaling pathway.Braz J Med Biol Res. 2020;53(10):e9849. doi: 10.1590/1414-431X20209849. Epub 2020 Sep 7. Braz J Med Biol Res. 2020. PMID: 32901689 Free PMC article.
References
-
- Rohde LE, Clausell N, Ribeiro JP, Goldraich L, Netto R, William Dec G, et al. Health outcomes in decompensated congestive heart failure: a comparison of tertiary hospitals in Brazil and United States. Int J Cardiol. 2005;102(1):71–77. - PubMed
-
- Butler J, Fonarow GC, Gheorghiade M. Strategies and opportunities for drug development in heart failure. JAMA. 2013;309(15):1593–1594. - PubMed
-
- Gheorghiade M, Vaduganathan M, Fonarow GC, Bonow RO. Rehospitalization for heart failure: problems and perspectives. J Am Coll Cardiol. 2013;61(4):391–403. - PubMed
-
- Dracup K, Walden JA, Stevenson LW, Brecht ML. Quality of life in patients with advanced heart failure. Pt 1J Heart Lung Transplant. 1992;11(2):273–279. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
