

Regional Nodal Irradiation in Early-Stage Breast Cancer
- PMID: 26200977
- PMCID: PMC4556358
- DOI: 10.1056/NEJMoa1415340
Regional Nodal Irradiation in Early-Stage Breast Cancer
Abstract
Background: Most women with breast cancer who undergo breast-conserving surgery receive whole-breast irradiation. We examined whether the addition of regional nodal irradiation to whole-breast irradiation improved outcomes.
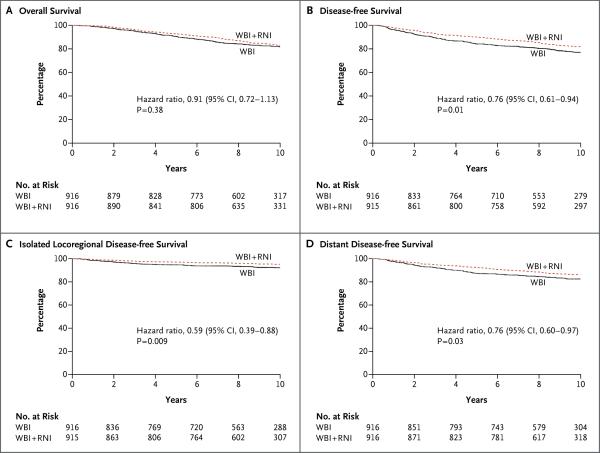
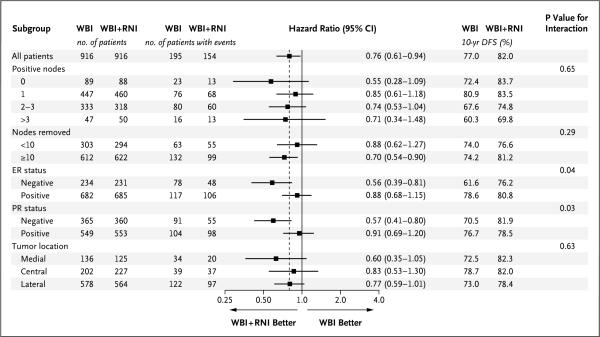
Methods: We randomly assigned women with node-positive or high-risk node-negative breast cancer who were treated with breast-conserving surgery and adjuvant systemic therapy to undergo either whole-breast irradiation plus regional nodal irradiation (including internal mammary, supraclavicular, and axillary lymph nodes) (nodal-irradiation group) or whole-breast irradiation alone (control group). The primary outcome was overall survival. Secondary outcomes were disease-free survival, isolated locoregional disease-free survival, and distant disease-free survival.
Results: Between March 2000 and February 2007, a total of 1832 women were assigned to the nodal-irradiation group or the control group (916 women in each group). The median follow-up was 9.5 years. At the 10-year follow-up, there was no significant between-group difference in survival, with a rate of 82.8% in the nodal-irradiation group and 81.8% in the control group (hazard ratio, 0.91; 95% confidence interval [CI], 0.72 to 1.13; P=0.38). The rates of disease-free survival were 82.0% in the nodal-irradiation group and 77.0% in the control group (hazard ratio, 0.76; 95% CI, 0.61 to 0.94; P=0.01). Patients in the nodal-irradiation group had higher rates of grade 2 or greater acute pneumonitis (1.2% vs. 0.2%, P=0.01) and lymphedema (8.4% vs. 4.5%, P=0.001).
Conclusions: Among women with node-positive or high-risk node-negative breast cancer, the addition of regional nodal irradiation to whole-breast irradiation did not improve overall survival but reduced the rate of breast-cancer recurrence. (Funded by the Canadian Cancer Society Research Institute and others; MA.20 ClinicalTrials.gov number, NCT00005957.).
Figures
Comment in
-
Nodal Irradiation after Breast-Cancer Surgery in the Era of Effective Adjuvant Therapy.N Engl J Med. 2015 Jul 23;373(4):379-81. doi: 10.1056/NEJMe1503608. N Engl J Med. 2015. PMID: 26200984 No abstract available.
-
Extra radiation to lymph nodes reduces breast cancer recurrence, studies show.BMJ. 2015 Jul 22;351:h4012. doi: 10.1136/bmj.h4012. BMJ. 2015. PMID: 26206999 No abstract available.
-
Breast cancer: rational use of regional nodal irradiation needed.Nat Rev Clin Oncol. 2015 Sep;12(9):501. doi: 10.1038/nrclinonc.2015.136. Epub 2015 Aug 4. Nat Rev Clin Oncol. 2015. PMID: 26241938 No abstract available.
-
[Regional nodal irradiation in early-stage breast cancer with 0-3 positive nodes].Strahlenther Onkol. 2015 Nov;191(11):889-91. doi: 10.1007/s00066-015-0897-0. Strahlenther Onkol. 2015. PMID: 26374451 German. No abstract available.
-
Regional Nodal Irradiation in Early-Stage Breast Cancer.N Engl J Med. 2015 Nov 5;373(19):1878-9. doi: 10.1056/NEJMc1510505. N Engl J Med. 2015. PMID: 26535517 No abstract available.
-
Regional Nodal Irradiation in Early-Stage Breast Cancer.N Engl J Med. 2015 Nov 5;373(19):1877-8. doi: 10.1056/NEJMc1510505. N Engl J Med. 2015. PMID: 26535518 No abstract available.
-
Proton Therapy for Breast Cancer: Getting to the Heart of the Matter.Int J Radiat Oncol Biol Phys. 2016 May 1;95(1):46-48. doi: 10.1016/j.ijrobp.2015.11.035. Int J Radiat Oncol Biol Phys. 2016. PMID: 27084624 No abstract available.
References
-
- Fisher B, Bauer M, Margolese R, et al. Five-year results of a randomized clinical trial comparing total mastectomy and segmental mastectomy with or without radiation in the treatment of breast cancer. N Engl J Med. 1985;312:665–73. - PubMed
-
- Veronesi U, Luini A, Del Vecchio M, et al. Radiotherapy after breast-preserving surgery in women with localized cancer of the breast. N Engl J Med. 1993;328:1587–91. - PubMed
-
- Clark RM, Whelan T, Levine M, et al. Randomized clinical trial of breast irradiation following lumpectomy and axillary dissection for node-negative breast cancer: an update. J Natl Cancer Inst. 1996;88:1659–64. - PubMed
-
- Ragaz J, Jackson SM, Le N, et al. Adjuvant radiotherapy and chemotherapy in node-positive premenopausal women with breast cancer. N Engl J Med. 1997;337:956–62. - PubMed
-
- Overgaard M, Hansen PS, Overgaard J, et al. Postoperative radiotherapy in high-risk premenopausal women with breast cancer who receive adjuvant chemotherapy: Danish Breast Cancer Cooperative Group 82b Trial. N Engl J Med. 1997;337:949–55. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical