

Long-Term Outcomes of Abdominal Aortic Aneurysm in the Medicare Population
- PMID: 26200979
- PMCID: PMC4532303
- DOI: 10.1056/NEJMoa1405778
Long-Term Outcomes of Abdominal Aortic Aneurysm in the Medicare Population
Abstract
Background: Randomized trials and observational studies have shown that perioperative morbidity and mortality are lower with endovascular repair of abdominal aortic aneurysm than with open repair, but the survival benefit is not sustained. In addition, concerns have been raised about the long-term risk of aneurysm rupture or the need for reintervention after endovascular repair.
Methods: We assessed perioperative and long-term survival, reinterventions, and complications after endovascular repair as compared with open repair of abdominal aortic aneurysm in propensity-score-matched cohorts of Medicare beneficiaries who underwent repair during the period from 2001 through 2008 and were followed through 2009.
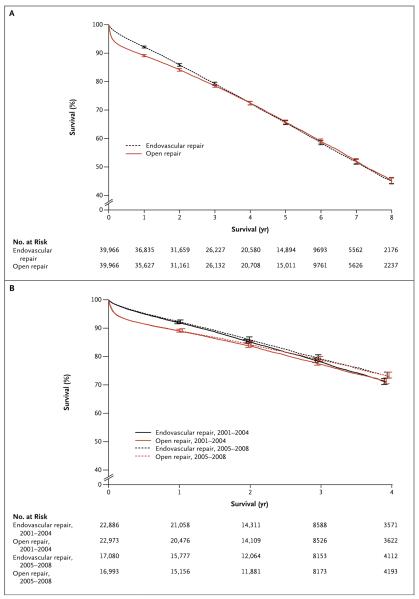
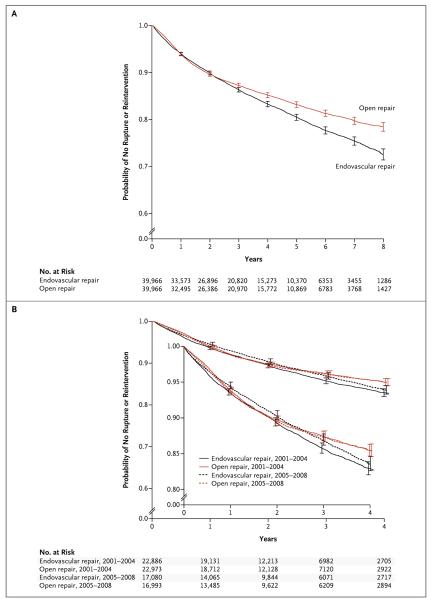
Results: We identified 39,966 matched pairs of patients who had undergone either open repair or endovascular repair. The overall perioperative mortality was 1.6% with endovascular repair versus 5.2% with open repair (P<0.001). From 2001 through 2008, perioperative mortality decreased by 0.8 percentage points among patients who underwent endovascular repair (P=0.001) and by 0.6 percentage points among patients who underwent open repair (P=0.01). The rate of conversion from endovascular to open repair decreased from 2.2% in 2001 to 0.3% in 2008 (P<0.001). The rate of survival was significantly higher after endovascular repair than after open repair through the first 3 years of follow-up, after which time the rates of survival were similar. Through 8 years of follow-up, interventions related to the management of the aneurysm or its complications were more common after endovascular repair, whereas interventions for complications related to laparotomy were more common after open repair. Aneurysm rupture occurred in 5.4% of patients after endovascular repair versus 1.4% of patients after open repair through 8 years of follow-up (P<0.001). The rate of total reinterventions at 2 years after endovascular repair decreased over time (from 10.4% among patients who underwent procedures in 2001 to 9.1% among patients who underwent procedures in 2007).
Conclusions: Endovascular repair, as compared with open repair, of abdominal aortic aneurysm was associated with a substantial early survival advantage that gradually decreased over time. The rate of late rupture was significantly higher after endovascular repair than after open repair. The outcomes of endovascular repair have been improving over time. (Funded by the National Institutes of Health.).
Figures
Comment in
-
Aortic disease: Endovascular vs. open AAA repair.Nat Rev Cardiol. 2015 Sep;12(9):500. doi: 10.1038/nrcardio.2015.122. Epub 2015 Aug 11. Nat Rev Cardiol. 2015. PMID: 26259936 No abstract available.
-
Long-Term Outcomes of Abdominal Aortic Aneurysm Repair.N Engl J Med. 2015 Nov 19;373(21):2088-9. doi: 10.1056/NEJMc1511634. N Engl J Med. 2015. PMID: 26581006 No abstract available.
-
Long-Term Outcomes of Abdominal Aortic Aneurysm Repair.N Engl J Med. 2015 Nov 19;373(21):2087-8. doi: 10.1056/NEJMc1511634. N Engl J Med. 2015. PMID: 26581007 No abstract available.
-
Long-Term Outcomes of Abdominal Aortic Aneurysm Repair.N Engl J Med. 2015 Nov 19;373(21):2088. doi: 10.1056/NEJMc1511634. N Engl J Med. 2015. PMID: 26581008 No abstract available.
-
Long-Term Outcomes of Abdominal Aortic Aneurysm Repair.N Engl J Med. 2015 Nov 19;373(21):2088. doi: 10.1056/NEJMc1511634. N Engl J Med. 2015. PMID: 26581009 No abstract available.
References
-
- Dua A, Kuy S, Lee CJ, Upchurch GR, Jr, Desai SS. Epidemiology of aortic aneurysm repair in the United States from 2000 to 2010. J Vasc Surg. 2014;59:1512–7. - PubMed
-
- Prinssen M, Verhoeven EL, Buth J, et al. A randomized trial comparing conventional and endovascular repair of abdominal aortic aneurysms. N Engl J Med. 2004;351:1607–18. - PubMed
-
- EVAR Trial Participants Endovascular aneurysm repair versus open repair in patients with abdominal aortic aneurysm (EVAR trial 1): randomised controlled trial. Lancet. 2005;365:2179–86. - PubMed
-
- Lederle FA, Freischlag JA, Kyriakides TC, et al. Outcomes following endovascular vs open repair of abdominal aortic aneurysm: a randomized trial. JAMA. 2009;302:1535–42. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical