

Deworming drugs for soil-transmitted intestinal worms in children: effects on nutritional indicators, haemoglobin, and school performance
- PMID: 26202783
- PMCID: PMC4523932
- DOI: 10.1002/14651858.CD000371.pub6
Deworming drugs for soil-transmitted intestinal worms in children: effects on nutritional indicators, haemoglobin, and school performance
Update in
-
Public health deworming programmes for soil-transmitted helminths in children living in endemic areas.Cochrane Database Syst Rev. 2019 Sep 11;9(9):CD000371. doi: 10.1002/14651858.CD000371.pub7. Cochrane Database Syst Rev. 2019. PMID: 31508807 Free PMC article.
Abstract
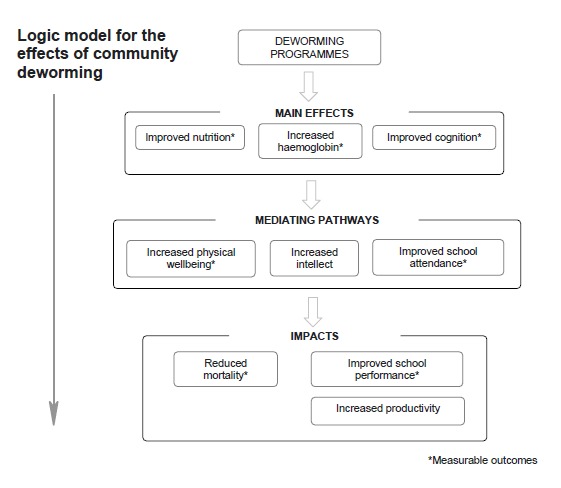
Background: The World Health Organization (WHO) recommends treating all school children at regular intervals with deworming drugs in areas where helminth infection is common. As the intervention is often claimed to have important health, nutrition, and societal effects beyond the removal of worms, we critically evaluated the evidence on benefits.
Objectives: To summarize the effects of giving deworming drugs to children to treat soil-transmitted helminths on weight, haemoglobin, and cognition; and the evidence of impact on physical well-being, school attendance, school performance, and mortality.
Search methods: We searched the Cochrane Infectious Diseases Group Specialized Register (14 April 2015); Cochrane Central Register of Controlled Trials (CENTRAL), published in the Cochrane Library (2015, Issue 4); MEDLINE (2000 to 14 April 2015); EMBASE (2000 to 14 April 2015); LILACS (2000 to 14 April 2015); the metaRegister of Controlled Trials (mRCT); and reference lists, and registers of ongoing and completed trials up to 14 April 2015.
Selection criteria: We included randomized controlled trials (RCTs) and quasi-RCTs comparing deworming drugs for soil-transmitted helminths with placebo or no treatment in children aged 16 years or less, reporting on weight, haemoglobin, and formal tests of intellectual development. We also sought data on school attendance, school performance, and mortality. We included trials that combined health education with deworming programmes.
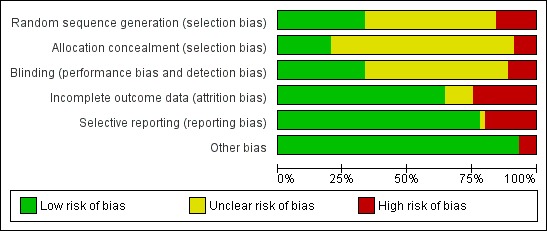
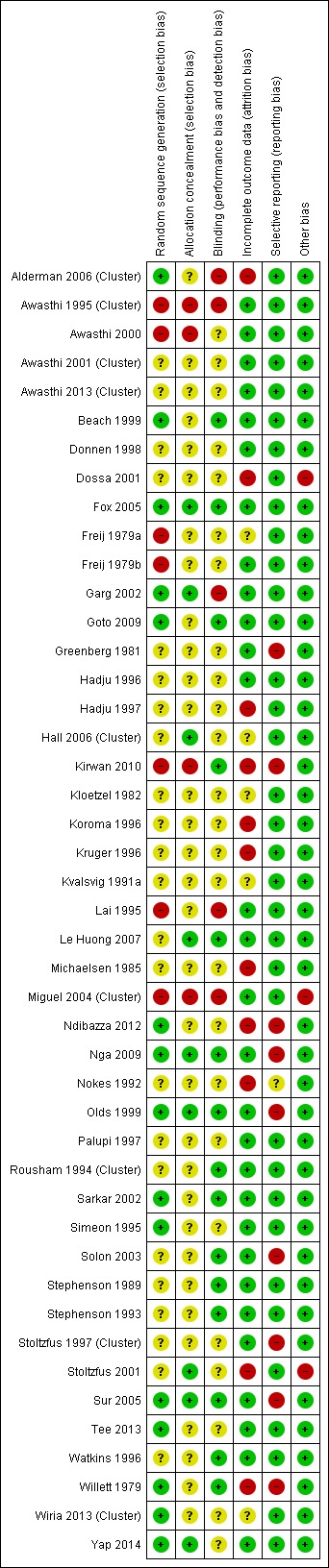
Data collection and analysis: At least two review authors independently assessed the trials, evaluated risk of bias, and extracted data. We analysed continuous data using the mean difference (MD) with 95% confidence intervals (CIs). Where data were missing, we contacted trial authors. We used outcomes at time of longest follow-up. The evidence quality was assessed using GRADE. This edition of the Cochrane Review adds the DEVTA trial from India, and draws on an independent analytical replication of a trial from Kenya.
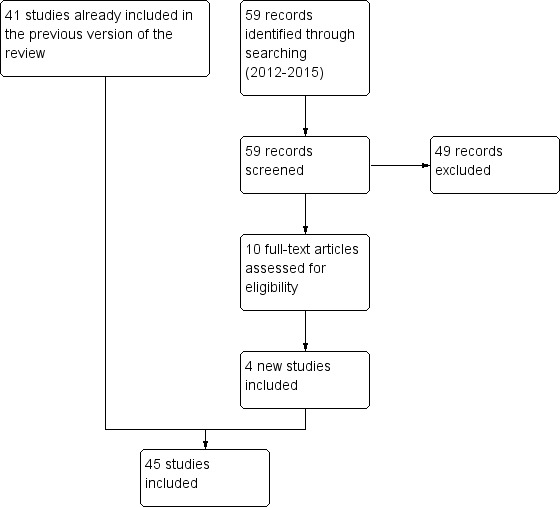
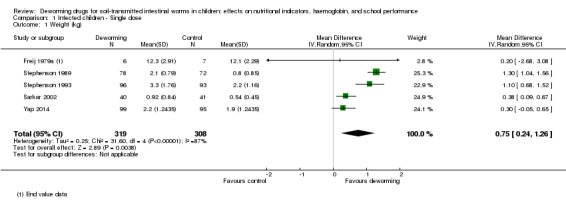
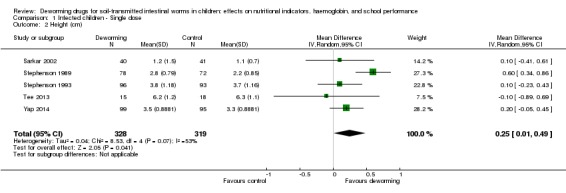
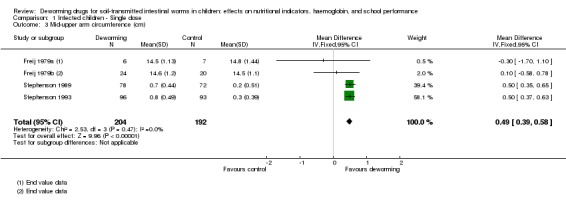
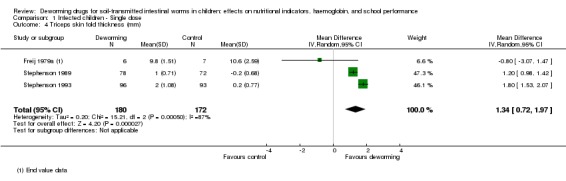
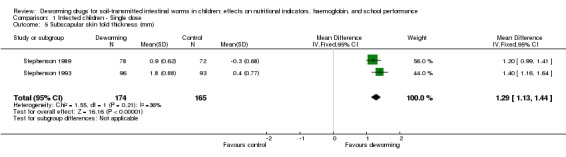
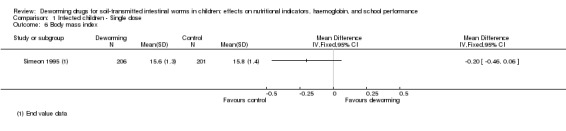
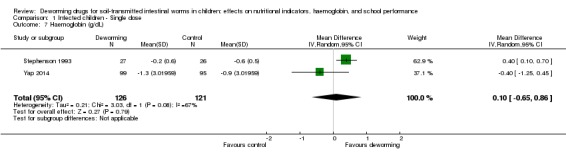
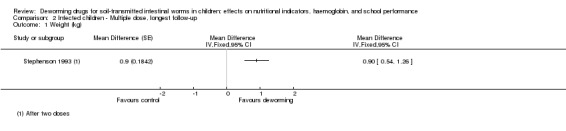
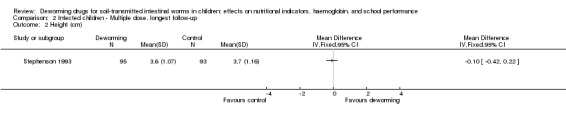
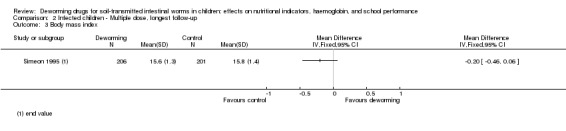
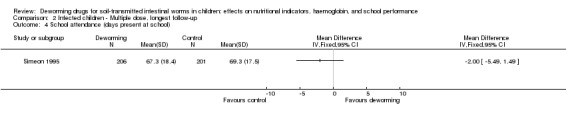
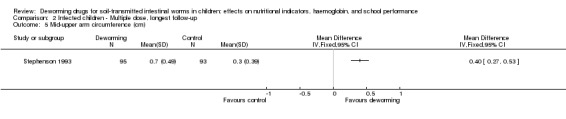
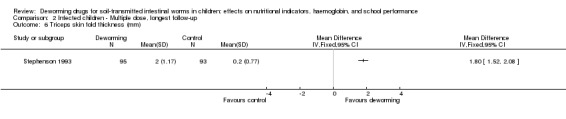
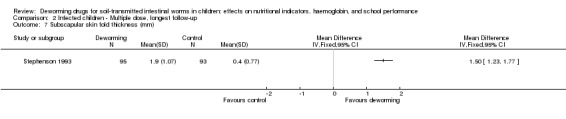
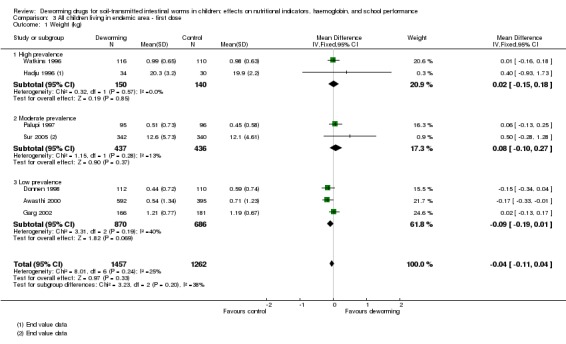
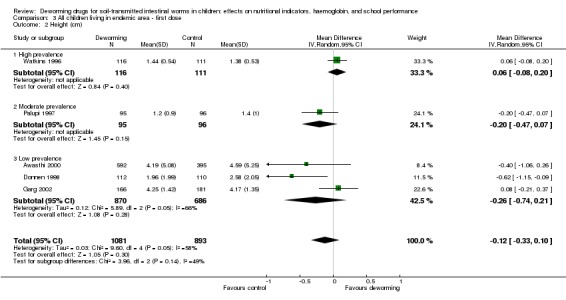
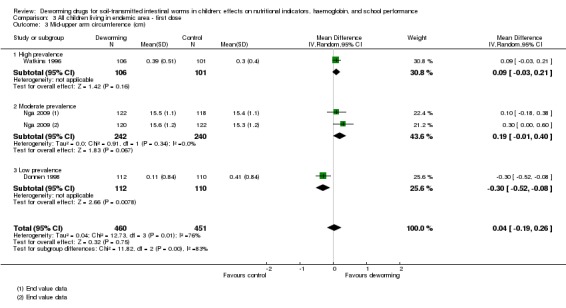
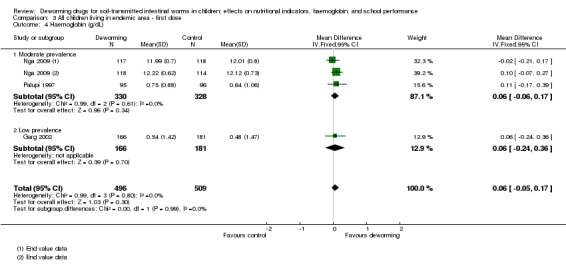
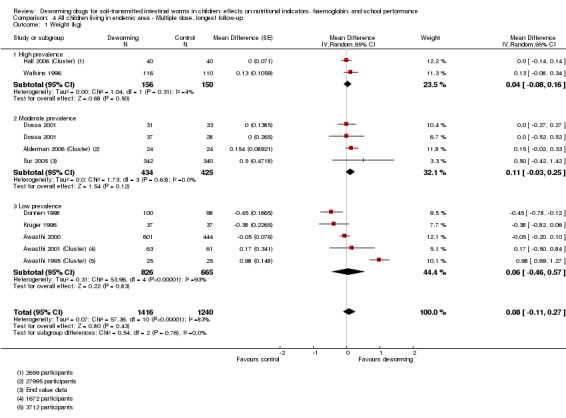
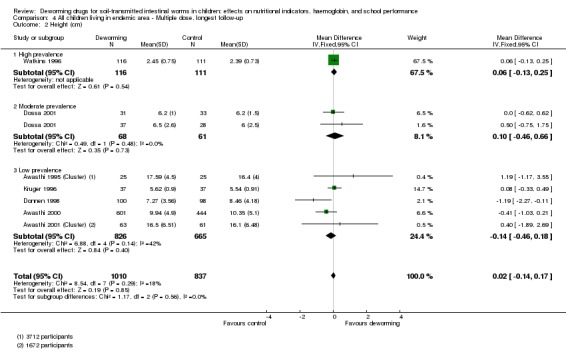
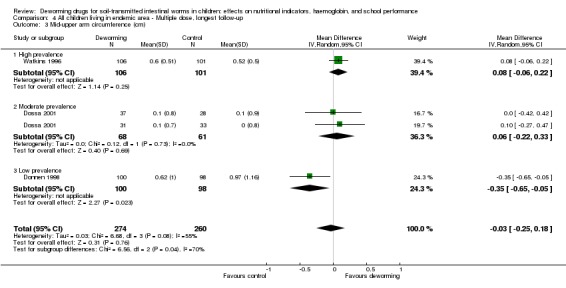
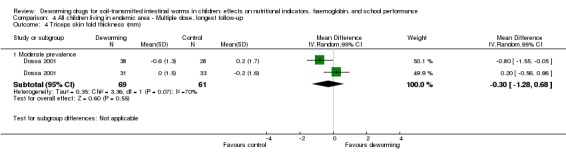
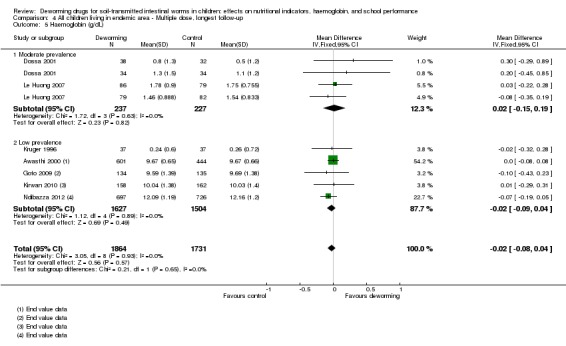
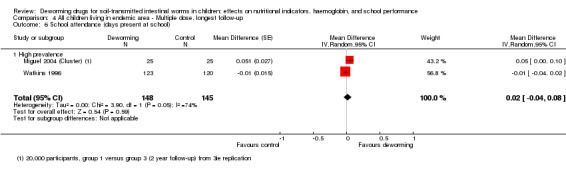
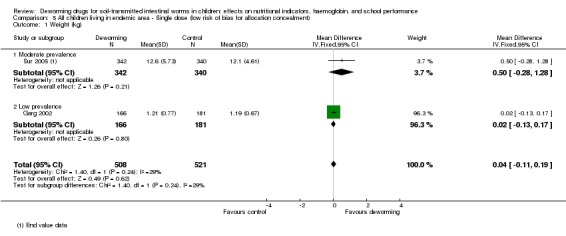
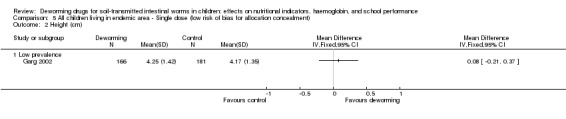
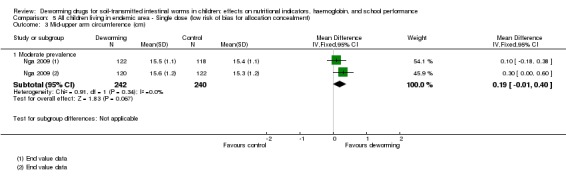
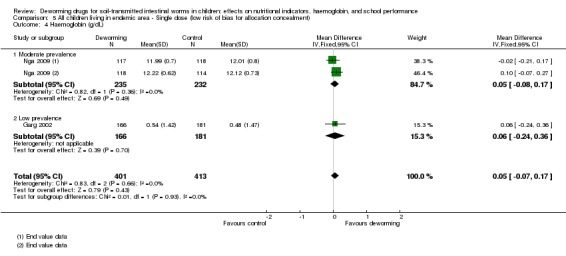
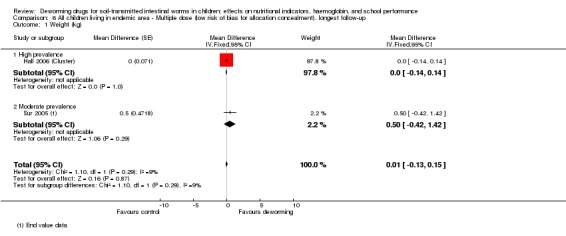
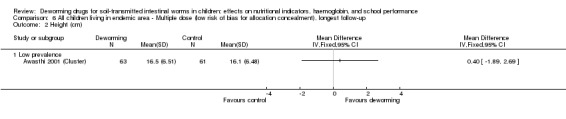
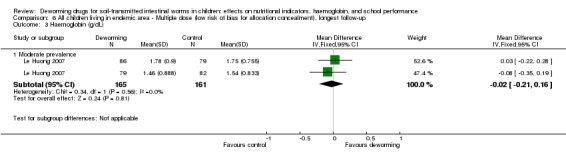
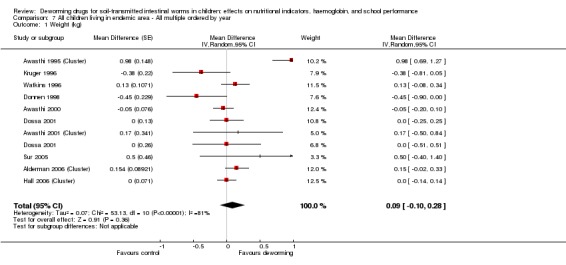
Main results: We identified 45 trials, including nine cluster-RCTs, that met the inclusion criteria. One trial evaluating mortality included over one million children, and the remaining 44 trials included a total of 67,672 participants. Eight trials were in children known to be infected, and 37 trials were carried out in endemic areas, including areas of high (15 trials), moderate (12 trials), and low prevalence (10 trials). Treating children known to be infectedTreating children known to be infected with a single dose of deworming drugs (selected by screening, or living in areas where all children are infected) may increase weight gain over the next one to six months (627 participants, five trials, low quality evidence). The effect size varied across trials from an additional 0.2 kg gain to 1.3 kg. There is currently insufficient evidence to know whether treatment has additional effects on haemoglobin (247 participants, two trials, very low quality evidence); school attendance (0 trials); cognitive functioning (103 participants, two trials, very low quality evidence), or physical well-being (280 participants, three trials, very low quality evidence). Community deworming programmesTreating all children living in endemic areas with a dose of deworming drugs probably has little or no effect on average weight gain (MD 0.04 kg less, 95% CI 0.11 kg less to 0.04 kg more; trials 2719 participants, seven trials, moderate quality evidence), even in settings with high prevalence of infection (290 participants, two trials). A single dose also probably has no effect on average haemoglobin (MD 0.06 g/dL, 95% CI -0.05 lower to 0.17 higher; 1005 participants, three trials, moderate quality evidence), or average cognition (1361 participants, two trials, low quality evidence).Similiarly, regularly treating all children in endemic areas with deworming drugs, given every three to six months, may have little or no effect on average weight gain (MD 0.08 kg, 95% CI 0.11 kg less to 0.27 kg more; 38,392 participants, 10 trials, low quality evidence). The effects were variable across trials; one trial from a low prevalence setting carried out in 1995 found an increase in weight, but nine trials carried out since then found no effect, including five from moderate and high prevalence areas.There is also reasonable evidence that regular treatment probably has no effect on average height (MD 0.02 cm higher, 95% CI 0.14 lower to 0.17 cm higher; 7057 participants, seven trials, moderate quality evidence); average haemoglobin (MD 0.02 g/dL lower; 95% CI 0.08 g/dL lower to 0.04 g/dL higher; 3595 participants, seven trials, low quality evidence); formal tests of cognition (32,486 participants, five trials, moderate quality evidence); exam performance (32,659 participants, two trials, moderate quality evidence); or mortality (1,005,135 participants, three trials, low quality evidence). There is very limited evidence assessing an effect on school attendance and the findings are inconsistent, and at risk of bias (mean attendance 2% higher, 95% CI 4% lower to 8% higher; 20,243 participants, two trials, very low quality evidence).In a sensitivity analysis that only included trials with adequate allocation concealment, there was no evidence of any effect for the main outcomes.
Authors' conclusions: Treating children known to have worm infection may have some nutritional benefits for the individual. However, in mass treatment of all children in endemic areas, there is now substantial evidence that this does not improve average nutritional status, haemoglobin, cognition, school performance, or survival.
Conflict of interest statement
This Cochrane Review is supported by a DFID grant aimed at ensuring the best possible systematic reviews, particularly Cochrane Reviews, are completed on topics relevant to the poor, particularly women, in low‐ and middle‐income countries. DFID does not participate in the selection of topics, in the conduct of the review, or in the interpretation of findings. The grant provides partial salary support for PG, SD, and the funds for the contract with Enhance Reviews Ltd.
PG receives additional salary support from the COUNTDOWN Research Consortium, which is funded by the DFID. COUNTDOWN is committed to trials and development of mass treatment programmes related to NTDs.
Figures
Update of
-
Deworming drugs for soil-transmitted intestinal worms in children: effects on nutritional indicators, haemoglobin and school performance.Cochrane Database Syst Rev. 2012 Nov 14;11:CD000371. doi: 10.1002/14651858.CD000371.pub5. Cochrane Database Syst Rev. 2012. Update in: Cochrane Database Syst Rev. 2015 Jul 23;(7):CD000371. doi: 10.1002/14651858.CD000371.pub6. PMID: 23152203 Updated.
Comment in
-
The end of the wormwars?Cochrane Database Syst Rev. 2016 Sep 27;9(9):ED000116. doi: 10.1002/14651858.ED000116. Cochrane Database Syst Rev. 2016. PMID: 27681359 Free PMC article. No abstract available.
References
References to studies included in this review
-
- Awasthi S, Peto R, Fletcher R, Glick H. Controlling parasitic infection in children under five years of age: giving albendazole in conjunction with an Indian government Vitamin A supplement program. Treating parasitic infestations in children [Monograph No. 3]. Philadelphia: International Clinical Epidemiology Network (INCLEN), 1995.
- Awasthi S, Peto R, Pande VK, Fletcher RH, Read S, Bundy DA. Effects of deworming on malnourished preschool children in India: an open‐labelled, cluster‐randomized trial. PLoS Neglected Tropical Diseases 2008;2(4):e223. - PMC - PubMed
-
- Awasthi S, Pande VK, Fletcher RS. Effectiveness and cost‐effectiveness of albendazole in improving nutritional status of pre‐school children in urban slums. Indian Pediatrics 2000;37(1):19‐29. - PubMed
-
- Awasthi S, Pande VK. Six‐monthly de‐worming in infants to study effects on growth. Indian Journal of Pediatrics 2001;68(9):823‐7. - PubMed
-
- Awasthi S, Peto R, Read S, Richards S, Pande V, Bundy DA, DEVTA team. Population de‐worming with 6‐monthly albendazole: DEVTA, a cluster‐randomised trial among 1 million preschool children in North India. [unpublished manuscript]. - PubMed
- University of Oxford and the United States Agency for International Development (USAID). Deworming and Enhanced Vitamin A Supplementation DEVTA Project (The DEVTA Trial). https://clinicaltrials.gov/ct2/show/NCT00222547 (accessed 23 February 2012).
References to studies excluded from this review
-
- Araujo RL, Araujo MB, Machado RD, Braga AA, Leite BV, Oliveira JR. Evaluation of a program to overcome vitamin A and iron deficiencies in areas of poverty in Minas Gerais, Brazil. Archivos Latinoamericanos de Nutrición 1987;37(1):9‐22. - PubMed
-
- Baird S, Hicks JH, Kremer M, Miguel E. Worms at Work: Long‐run Impacts of Child Health Gains. http://eml.berkeley.edu//˜emiguel/pdfs/miguel_wormsatwork.pdf (accessed 10 July 2015. - PMC - PubMed
-
- Beasley NM, Tomkins AM, Hall A, Kihamia CM, Lorri W, Nduma B, et al. The impact of population level deworming on the haemoglobin levels of schoolchildren in Tanga, Tanzania. Tropical Medicine and International Health 1999;4(11):744‐50. - PubMed
-
- Bhargava A, Jukes M, Lambo J, Kihamia CM, Lorri W, Nokes C, et al. Anthelmintic treatment improves the hemoglobin and serum ferritin concentrations of Tanzanian schoolchildren. Food and Nutrition Bulletin 2003;24(4):332‐42. - PubMed
-
- Bhutta Z, Klemm R, Shahid F, Rizvi A, Rah JH, Christian P. Treatment response to iron and folic acid alone is the same as with multivitamins and/or anthelminthics in severely anemic 6‐ to 24‐month‐old children. Journal of Nutrition 2009;139(8):1568‐74. - PubMed
References to ongoing studies
-
- Alam MM, Principal Investigator, ICDDR, B: Centre for Health and Population Research. Relative efficacy of two regimens of ante‐helminthic treatment. ClinicalTrials.gov identifier: NCT00367627.
Additional references
-
- International Initiative for Impact Evaluation. 3ie replication paper 3: Part 1 and 2. http://www.3ieimpact.org/en/publications/3ie‐replication‐paper‐series/3i... (accessed 5 June 2015).
-
- Aiken AM, Davey C, Hargreaves JR, Hayes RJ. Reanalysis of health and educational impacts of a school‐based deworming program in western Kenya: Part 1, pure replication, 3ie Replication Paper 3, Part 1. Washington, DC: International Initiative for Impact Evaluation (3ie). http://www.3ieimpact.org/media/filer_public/2015/01/07/3ie_rps3_worms_re... (accessed 10 July 2015).
-
- Aiken A, Davey C, Hargreaves J, Hayes R. Re‐analysis of health and educational impacts of a school‐based deworming program in western Kenya: a pure replication. International Journal of Epidemiology 2015; DOI 10.1093/ije/dyv127.. - PMC - PubMed
-
- Anderson RM, May RM. Infectious Diseases of Humans: Dynamics and Control. Oxford: Oxford University Press, 1991.
References to other published versions of this review
-
- Taylor‐Robinson DC, Maayan N, Soares‐Weiser K, Donegan S, Garner P. Deworming drugs for soil‐transmitted intestinal worms in children: effects on nutritional indicators, haemoglobin and school performance. Cochrane Database of Systematic Reviews 2012, Issue 11. [DOI: 10.1002/14651858.CD000371.pub5] - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous