

Adverse events associated with poor neurological outcome during targeted temperature management and advanced critical care after out-of-hospital cardiac arrest
- PMID: 26202789
- PMCID: PMC4511983
- DOI: 10.1186/s13054-015-0991-9
Adverse events associated with poor neurological outcome during targeted temperature management and advanced critical care after out-of-hospital cardiac arrest
Abstract
Introduction: The aim of this study was to investigate the association of adverse events (AEs) during targeted temperature management (TTM) and other AEs and concomitant treatments during the advanced critical care period with poor neurological outcome at hospital discharge in adult out-of-hospital cardiac arrest (OHCA) patients.
Methods: This was a retrospective study using Korean Hypothermia Network registry data of adult OHCA patients treated with TTM in 24 teaching hospitals throughout South Korea from 2007 to 2012. Demographic characteristics, resuscitation and post-resuscitation variables, AEs, and concomitant treatments during TTM and the advanced critical care were collected. The primary outcome was poor neurological outcome, defined as a cerebral performance category (CPC) score of 3-5 at hospital discharge. The AEs and concomitant treatments were individually entered into the best multivariable predictive model of poor neurological outcome to evaluate the associations between each variable and outcome.
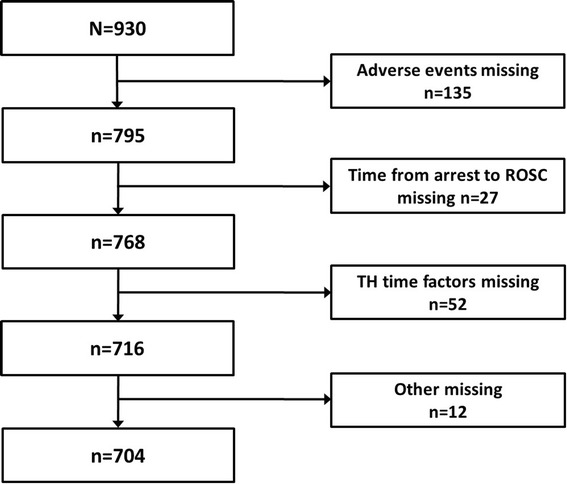
Results: A total of 930 patients, including 704 for whom a complete dataset of AEs and covariates was available for multivariable modeling, were included in the analysis; 476 of these patients exhibited poor neurological outcome [CPC 3 = 50 (7.1%), CPC 4 = 214 (30.4%), and CPC 5 = 212 (30.1%)]. Common AEs included hyperglycemia (45.6%), hypokalemia (31.3%), arrhythmia (21.3%) and hypotension (29%) during cooling, and hypotension (21.6%) during rewarming. Bleeding (5%) during TTM was a rare AE. Common AEs during the advanced critical care included pneumonia (39.6%), myoclonus (21.9%), seizures (21.7%) and hypoglycemia within 72 hours (23%). After adjusting for independent predictors of outcome, cooling- and rewarming-related AEs were not significantly associated with poor neurological outcome. However, sepsis, myoclonus, seizure, hypoglycemia within 72 hours and anticonvulsant use during the advanced critical care were associated with poor neurological outcome [adjusted odds ratios (95% confidence intervals) of 3.12 (1.40-6.97), 3.72 (1.93-7.16), 4.02 (2.04-7.91), 2.03 (1.09-3.78), and 1.69 (1.03-2.77), respectively]. Alternatively, neuromuscular blocker use was inversely associated with poor neurological outcome (0.48 [0.28-0.84]).
Conclusions: Cooling- and rewarming-related AEs were not associated with poor neurological outcome at hospital discharge. Sepsis, myoclonus, seizure, hypoglycemia within 72 hours and anticonvulsant use during the advanced critical care period were associated with poor neurological outcome at hospital discharge in our study.
Figures
References
-
- Ro YS, Shin SD, Song KJ, Lee EJ, Kim JY, Ahn KO, et al. A trend in epidemiology and outcomes of out-of-hospital cardiac arrest by urbanization level: a nationwide observational study from 2006 to 2010 in South Korea. Resuscitation. 2013;84:547–57. doi: 10.1016/j.resuscitation.2012.12.020. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
