

Importance of perforating vessels in nipple-sparing mastectomy: an anatomical description
- PMID: 26203275
- PMCID: PMC4507458
- DOI: 10.2147/BCTT.S78705
Importance of perforating vessels in nipple-sparing mastectomy: an anatomical description
Abstract
Background: Nipple-sparing mastectomy (NSM), understood as an oncologically valid procedure, is relatively new, and is an evolution of traditional mastectomy, particularly in relation to breast-conserving surgery. The anterior perforating branches are responsible for the cutaneous vascularization of the breast skin, and their preservation is a fundamental step to avoid possible postoperative necrosis. Therefore, evaluating the potential complications of cancer-related reconstructive surgical procedures such as NSM, both the distance of the tumoral lesion from the skin and the surgical incision site should be carefully considered. The preferred site of incision corresponds to the inframammary fold or possibly the periareolar area.
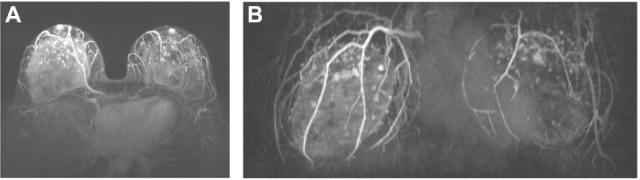
Methods: We retrospectively reviewed 113 patients who underwent NSM from January 2005 to October 2012 to evaluate skin complications. The anatomical study was performed by magnetic resonance imaging of the breast.
Results: Only one of the 113 women who had undergone a NSM procedure had total necrosis (0.9%) and six patients had partial necrosis (5.8%) of the nipple-areola complex.
Keywords: breast; breast anatomy; breast perforating vessels; magnetic resonance imaging; nipple-sparing mastectomy.
Figures

References
-
- Rusby JE, Smith BL, Gui GPH. Nipple-sparing mastectomy. Br J Surg. 2010;97:305–316. - PubMed
-
- Moyer HR, Ghazi B, Daniel JR, Gasgarth R, Carlson GW. Nipple-sparing mastectomy – technical aspects and aesthetic outcomes. Ann Plast Surg. 2012;68:446–450. - PubMed
-
- Petit JY, Veronesi U, Orecchia R, et al. Nipple sparing mastectomy with nipple areola intraoperative radiotherapy: one thousand and one cases of a five years’ experience at the European institute of Oncology of Milan (EIO) Breast Cancer Res Treat. 2009;117:333–338. - PubMed
-
- Chand M, Swan MC, Horlock N, Royle G. Preservation of the lateral thoracic vein in axillary dissection – its role in breast reconstruction using the DIEP flap. Breast. 2009;18:69–70. - PubMed
LinkOut - more resources
Full Text Sources
