

Viral Hepatitis Surveillance--India, 2011-2013
- PMID: 26203629
- PMCID: PMC4584861
- DOI: 10.15585/mmwr.mm6428a3
Viral Hepatitis Surveillance--India, 2011-2013
Abstract
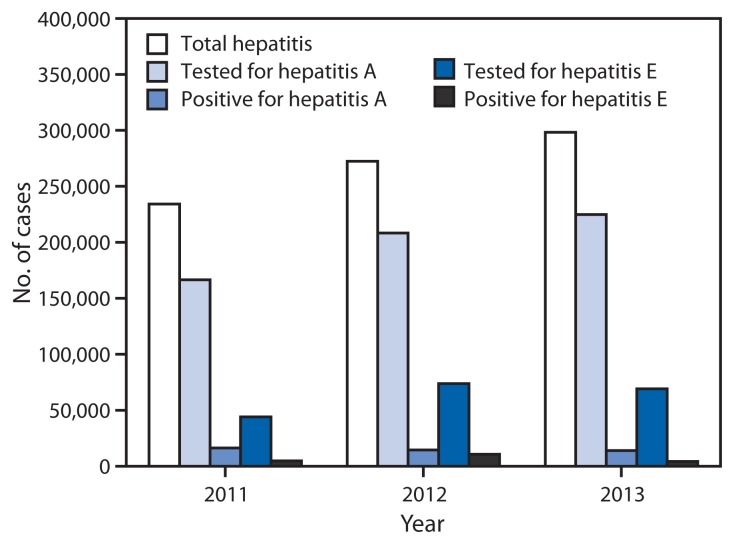
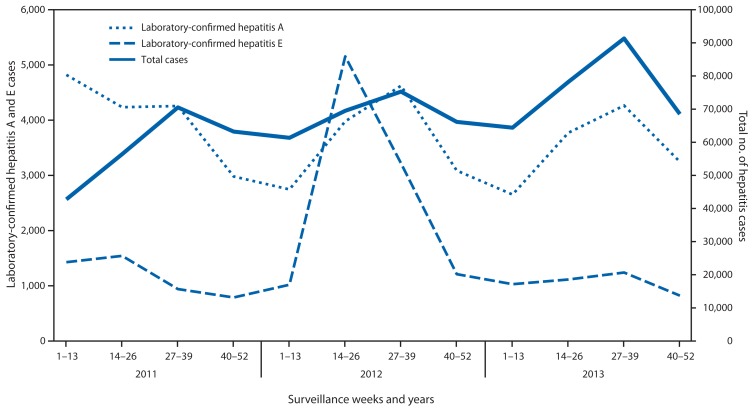
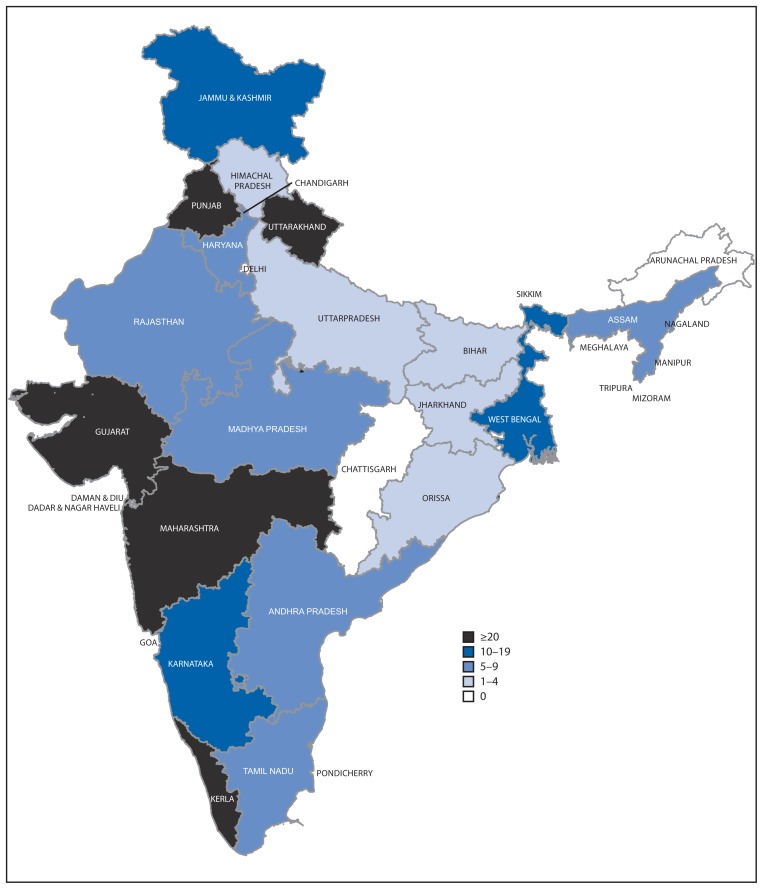
The burden of viral hepatitis in India is not well characterized. In 2009, the national Integrated Disease Surveillance Programme (IDSP) began conducting surveillance across all Indian states for epidemic-prone diseases, including foodborne and waterborne forms of viral hepatitis (e.g., hepatitis A and E). Information on outbreaks of all forms of viral hepatitis, including A, B, C, and E, also is collected. This report summarizes viral hepatitis surveillance and outbreak data reported to IDSP during 2011-2013. During this period, 804,782 hepatitis cases and 291 outbreaks were reported; the virus type was unspecified in 92% of cases. Among 599,605 cases tested for hepatitis A, 44,663 (7.4%) were positive, and among 187,040 tested for hepatitis E, 19,508 (10.4%) were positive. At least one hepatitis outbreak report was received from 23 (66%) of 35 Indian states. Two-thirds of outbreaks were reported from rural areas. Among 163 (56%) outbreaks with known etiology, 78 (48%) were caused by hepatitis E, 54 (33%) by hepatitis A, 19 (12%) by both hepatitis A and E, and 12 (7%) by hepatitis B or hepatitis C. Contaminated drinking water was the source of most outbreaks. Improvements in water quality and sanitation as well as inclusion of hepatitis A vaccine in childhood immunization programs should be considered to reduce the public health burden of hepatitis in India. Efforts to decrease the proportion of cases for which the etiology is unspecified, including expanding the IDSP to support hepatitis B and C testing, might help further elucidate the epidemiology of these diseases.
Figures
References
-
- John TJ, Dandona L, Sharma VP, Kakkar M. Continuing challenge of infectious diseases in India. Lancet. 2011;377:252–69. - PubMed
-
- Batham A, Gupta MA, Rastogi P, Garg S, Sreenivas V, Puliyel JM. Calculating prevalence of hepatitis B in India: using population weights to look for publication bias in conventional meta-analysis. Indian J Pediatr. 2009;76:1247–57. - PubMed
-
- Mukhopadhyaya A. Hepatitis C in India. J Biosci. 2008;33:465–73. - PubMed
-
- Suresh K. Integrated Diseases Surveillance Project (IDSP) through a consultant’s lens. Indian J Public Health. 2008;52:136–43. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
