

Acceptability of delivery modes for lifestyle advice in a large scale randomised controlled obesity prevention trial
- PMID: 26205958
- PMCID: PMC4513385
- DOI: 10.1186/s12889-015-1995-8
Acceptability of delivery modes for lifestyle advice in a large scale randomised controlled obesity prevention trial
Abstract
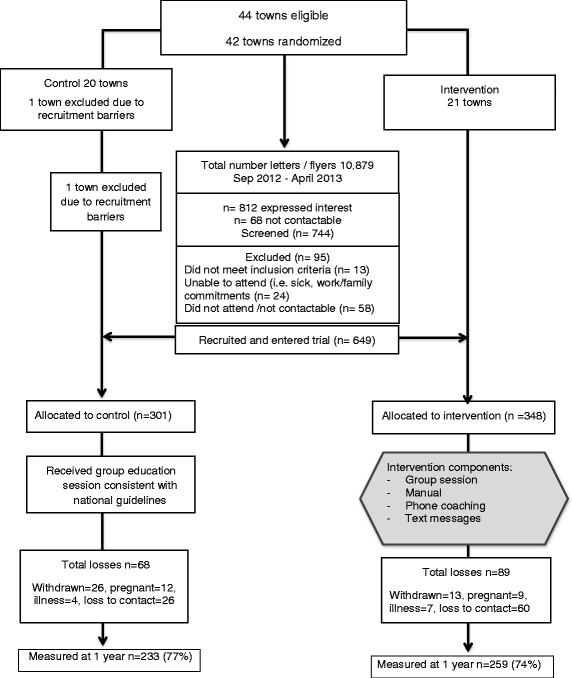
Background: Preventing obesity is an international health priority and women living in rural communities are at an increased risk of weight gain. Lifestyle programs are needed as part of a comprehensive approach to prevent obesity. Evaluation provides a unique opportunity to investigate and inform improvements in lifestyle program implementation strategies. The Healthy Lifestyle Program for rural women (HeLP-her Rural) is a large scale, cluster randomized control trial, targeting the prevention of weight gain. This program utilises multiple delivery modes for simple lifestyle advice (group sessions, phone coaching, text messages, and an interactive program manual). Here, we describe the acceptability of these various delivery modes.
Methods: A mixed-method process evaluation was undertaken measuring program fidelity, recruitment strategies, dose delivered, program acceptability and contextual factors influencing program implementation. Data collection methodologies included qualitative semi-structured interviews for a sub-group of intervention participants [n = 28] via thematic analysis and quantitative methods (program checklists and questionnaires [n = 190]) analysed via chi square and t-tests.
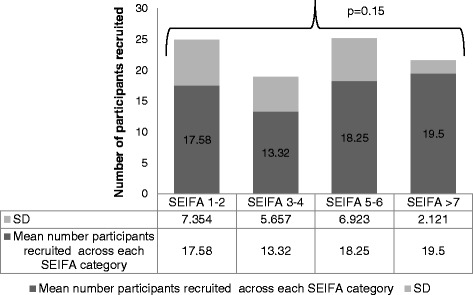
Results: We recruited 649 women from 41 rural townships into the HeLP-her Rural program with high levels of program fidelity, dose delivered and acceptability. Participants were from low socioeconomic townships and no differences were detected between socioeconomic characteristics and the number of participants recruited across the towns (p = 0.15). A face-to-face group session was the most commonly reported preferred delivery mode for receiving lifestyle advice, followed by text messages and phone coaching. Multiple sub-themes emerged to support the value of group sessions which included: promoting of a sense of belonging, mutual support and a forum to share ideas. The value of various delivery modes was influenced by participant's various needs and learning styles.
Conclusion: This comprehensive evaluation reveals strong implementation fidelity and high levels of dose delivery. We demonstrate reach to women from relatively low income rural townships and highlight the acceptability of low intensity healthy lifestyle programs with mixed face-to-face and remote delivery modes in this population. Group education sessions were the most highly valued component of the intervention, with at least one face-to-face session critical to successful program implementation. However, lifestyle advice via multiple delivery modes is recommended to optimise program acceptability and ultimately effectiveness.
Trial registry: Australia & New Zealand Clinical Trial Registry. Trial number ACTRN12612000115831, date of registration 24/01/2012.
Figures
Similar articles
-
Evaluation of a large healthy lifestyle program: informing program implementation and scale-up in the prevention of obesity.Implement Sci. 2016 Nov 24;11(1):151. doi: 10.1186/s13012-016-0521-4. Implement Sci. 2016. PMID: 27881146 Free PMC article.
-
Effectiveness and implementation of an obesity prevention intervention: the HeLP-her Rural cluster randomised controlled trial.BMC Public Health. 2014 Jun 16;14:608. doi: 10.1186/1471-2458-14-608. BMC Public Health. 2014. PMID: 24930478 Free PMC article. Clinical Trial.
-
Engaging rural women in healthy lifestyle programs: insights from a randomized controlled trial.Trials. 2015 Sep 16;16:413. doi: 10.1186/s13063-015-0860-5. Trials. 2015. PMID: 26377190 Free PMC article. Clinical Trial.
-
Process evaluations of early childhood obesity prevention interventions delivered via telephone or text messages: a systematic review.Int J Behav Nutr Phys Act. 2021 Jan 9;18(1):10. doi: 10.1186/s12966-020-01074-8. Int J Behav Nutr Phys Act. 2021. PMID: 33422066 Free PMC article.
-
Lifestyle physical activity interventions. History, short- and long-term effects, and recommendations.Am J Prev Med. 1998 Nov;15(4):398-412. doi: 10.1016/s0749-3797(98)00084-1. Am J Prev Med. 1998. PMID: 9838980 Review.
Cited by
-
Ethnographic methods for process evaluations of complex health behaviour interventions.Trials. 2016 May 4;17(1):232. doi: 10.1186/s13063-016-1340-2. Trials. 2016. PMID: 27142662 Free PMC article.
-
The feasibility of progressive resistance training in women with polycystic ovary syndrome: a pilot randomized controlled trial.BMC Sports Sci Med Rehabil. 2016 May 11;8:14. doi: 10.1186/s13102-016-0039-8. eCollection 2016. BMC Sports Sci Med Rehabil. 2016. PMID: 27175282 Free PMC article.
-
Tobacco use among Appalachian adolescents: An urgent need for virtual scale out of effective interventions.Tob Prev Cessat. 2022 Nov 4;8:39. doi: 10.18332/tpc/155331. eCollection 2022. Tob Prev Cessat. 2022. PMID: 36404952 Free PMC article.
-
Participants' Engagement With Telephone Support Interventions to Promote Healthy Feeding Practices and Obesity-Protective Behaviours for Infant Obesity Prevention.Front Endocrinol (Lausanne). 2022 May 2;13:868944. doi: 10.3389/fendo.2022.868944. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 35586630 Free PMC article.
-
Insights for dementia risk reduction among lower SES adults in OECD countries: scoping review of interventions targeting multiple common health risk factors.Int J Equity Health. 2025 Feb 24;24(1):52. doi: 10.1186/s12939-025-02386-6. Int J Equity Health. 2025. PMID: 39994664 Free PMC article.
References
-
- Australian Government National Preventative Health Taskforce. Australia: the healthiest country by 2020. Available: http://www.health.gov.au/internet/preventativehealth/publishing. Accessed June 28th, 2012.
-
- Australian Longitudinal Study on Women’s Health. Australian women and their weight - a growing problem. Available at: http://www.alswh.org.au/publications-and-reports/annual-reports. Accessed June 4th, 2012.
-
- Janus ED, Laatikainen T, Dunbar JA, Kilkkinen A, Bunker SJ, Philpot B, et al. Overweight, obesity and metabolic syndrome in rural southeastern Australia. Med J Aust. 2007;187(3):147–52. - PubMed
-
- Cleland V, Hume C, Crawford D, Timperio A, Hesketh K, Baur L, et al. Urban–rural comparison of weight status among women and children living in socioeconomically disadvantaged neighbourhoods. Med J Australia. 2010;192(3):137. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
