

Sacrospinous hysteropexy versus vaginal hysterectomy with suspension of the uterosacral ligaments in women with uterine prolapse stage 2 or higher: multicentre randomised non-inferiority trial
- PMID: 26206451
- PMCID: PMC4512203
- DOI: 10.1136/bmj.h3717
Sacrospinous hysteropexy versus vaginal hysterectomy with suspension of the uterosacral ligaments in women with uterine prolapse stage 2 or higher: multicentre randomised non-inferiority trial
Abstract
Objective: To investigate whether uterus preserving vaginal sacrospinous hysteropexy is non-inferior to vaginal hysterectomy with suspension of the uterosacral ligaments in the surgical treatment of uterine prolapse.
Design: Multicentre randomised controlled non-blinded non-inferiority trial.
Setting: 4 non-university teaching hospitals, the Netherlands.
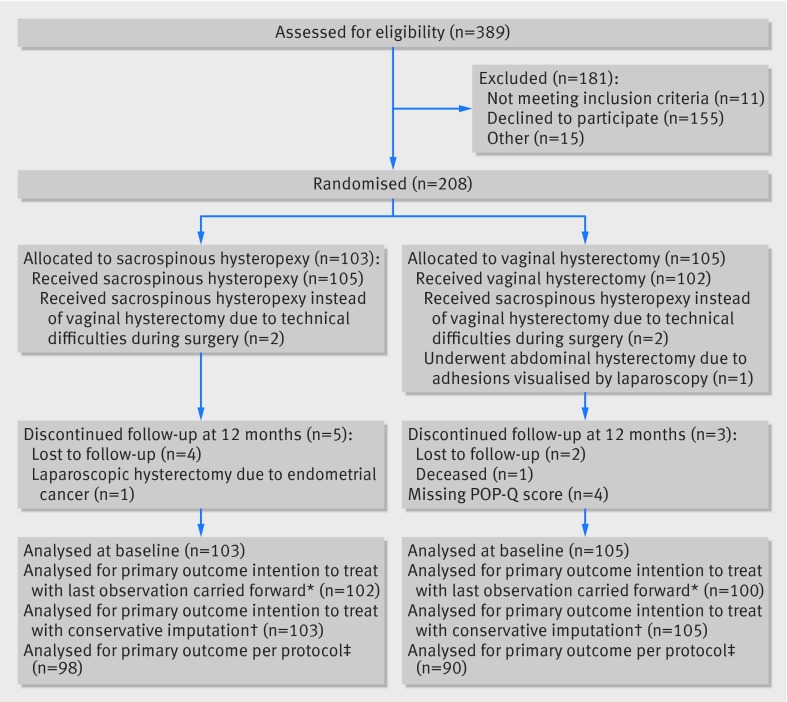
Participants: 208 healthy women with uterine prolapse stage 2 or higher requiring surgery and no history of pelvic floor surgery.
Interventions: Treatment with sacrospinous hysteropexy or vaginal hysterectomy with suspension of the uterosacral ligaments. The predefined non-inferiority margin was an increase in surgical failure rate of 7%.
Main outcome measures: Primary outcome was recurrent prolapse stage 2 or higher of the uterus or vaginal vault (apical compartment) evaluated by the pelvic organ prolapse quantification system in combination with bothersome bulge symptoms or repeat surgery for recurrent apical prolapse at 12 months' follow-up. Secondary outcomes were overall anatomical recurrences, including recurrent anterior compartment (bladder) and/or posterior compartment (bowel) prolapse, functional outcome, complications, hospital stay, postoperative recovery, and sexual functioning.
Results: Sacrospinous hysteropexy was non-inferior for anatomical recurrence of the apical compartment with bothersome bulge symptoms or repeat surgery (n=0, 0%) compared with vaginal hysterectomy with suspension of the uterosacral ligaments (n=4, 4.0%, difference -3.9%, 95% confidence interval for difference -8.6% to 0.7%). At 12 months, overall anatomical recurrences, functional outcome, quality of life, complications, hospital stay, measures on postoperative recovery, and sexual functioning did not differ between the two groups. Five serious adverse events were reported during hospital stay. None was considered to be related to the type of surgery.
Conclusions: Uterus preservation by sacrospinous hysteropexy was non-inferior to vaginal hysterectomy with suspension of the uterosacral ligaments for surgical failure of the apical compartment at 12 months' follow-up.
Trial registration: trialregister.nl NTR1866.
© Detollenaere et al 2015.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
References
-
- Slieker-ten Hove MC, Pool-Goudzwaard AL, Eijkemans MJ, Steegers-Theunissen RP, Burger CW, Vierhout ME. The prevalence of pelvic organ prolapse symptoms and signs and their relation with bladder and bowel disorders in a general female population. Int Urogynecol J Pelvic Floor Dysfunct 2009;20:1037-45. - PMC - PubMed
-
- Olsen AL, Smith VJ, Bergstrom JO, Colling JC, Clark AL. Epidemiology of surgically managed pelvic organ prolapse and urinary incontinence. Obstet Gynecol 1997;89:501-6. - PubMed
-
- De Boer TA, Slieker-ten Hove MC, Burger CW, Kluivers KB, Vierhout ME. The prevalence and factors associated with previous surgery for pelvic organ prolapse and or urinary incontinence in a cross sectional study in the Netherlands. Eur J Obstet Gynecol Reprod Biol 2011;158:343-9. - PubMed
-
- Jha S, Moran P. The UK national prolapse survey: 5 years on. Int Urogynecol J 2011;22:517-28. - PubMed
-
- Vanspauwen R, Seman E, Dwyer P. Survey of current management of prolapse in Australia and New Zealand. Aust N Z J Obstet Gynaecol 2010;50:262-7. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical