

Number of Lymph Nodes Removed and Survival after Gastric Cancer Resection: An Analysis from the US Gastric Cancer Collaborative
- PMID: 26206635
- PMCID: PMC4654942
- DOI: 10.1016/j.jamcollsurg.2015.04.024
Number of Lymph Nodes Removed and Survival after Gastric Cancer Resection: An Analysis from the US Gastric Cancer Collaborative
Abstract
Background: Examination of at least 16 lymph nodes (LNs) has been traditionally recommended during gastric adenocarcinoma resection to optimize staging, but the impact of this strategy on survival is uncertain. Because recent randomized trials have demonstrated a therapeutic benefit from extended lymphadenectomy, we sought to investigate the impact of the number of LNs removed on prognosis after gastric adenocarcinoma resection.
Study design: We analyzed patients who underwent gastrectomy for gastric adenocarcinoma from 2000 to 2012, at 7 US academic institutions. Patients with M1 disease or R2 resections were excluded. Disease-specific survival (DSS) was calculated using the Kaplan-Meier method and compared using log-rank and Cox regression analyses.
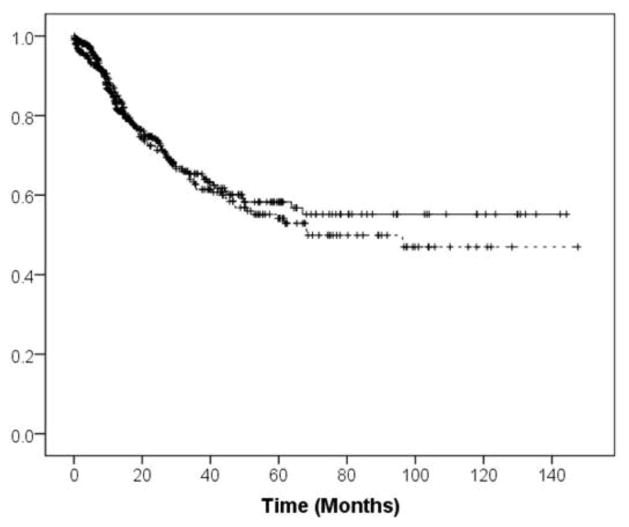
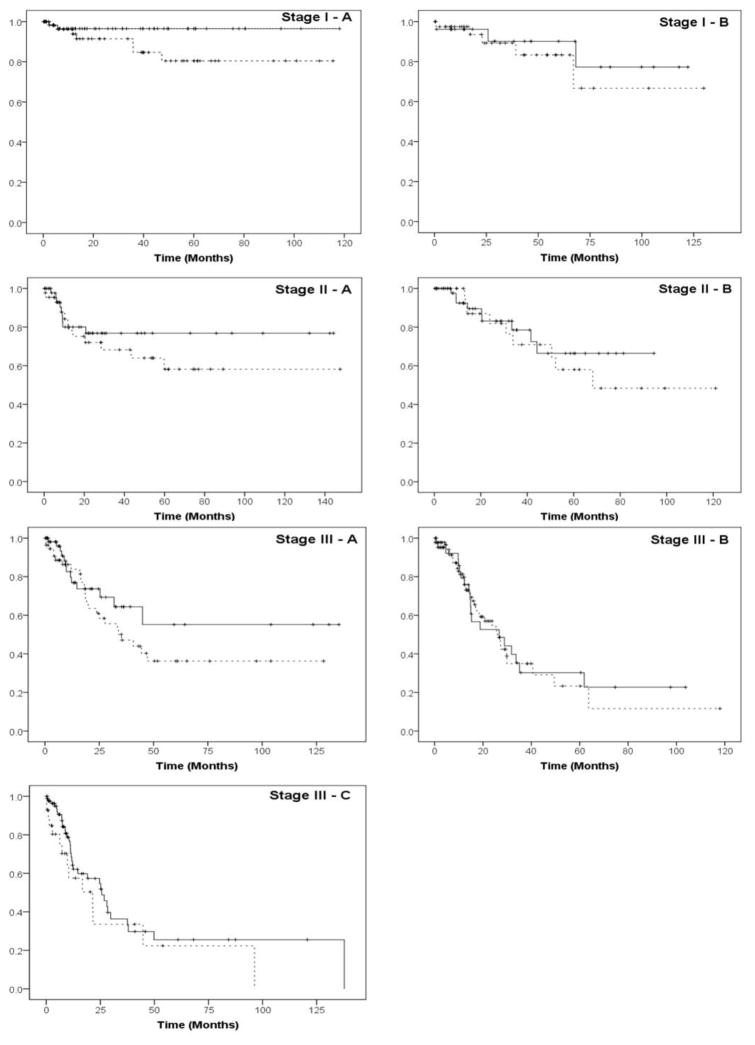
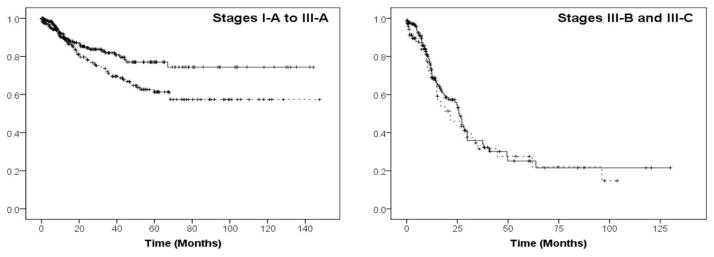
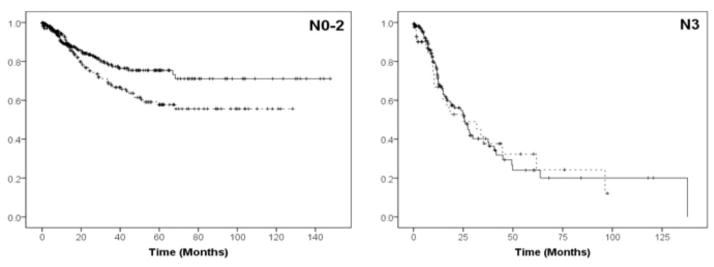
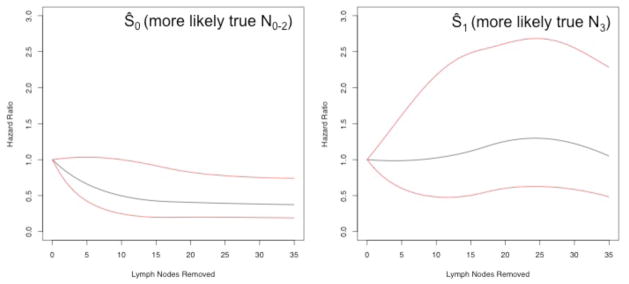
Results: Of 742 patients, 257 (35%) had 7 to 15 LNs removed and 485 (65%) had ≥16 LNs removed. Disease-specific survival was not significantly longer after removal of ≥16 vs 7 to 15 LNs (10-year survival, 55% vs 47%, respectively; p = 0.53) for the entire cohort, but was significantly improved in the subset of patients with stage IA to IIIA (10-year survival, 74% vs 57%, respectively; p = 0.018) or N0-2 disease (72% vs 55%, respectively; p = 0.023). Similarly, for patients who were classified to more likely be "true N0-2," based on frequentist analysis incorporating both the number of positive and of total LNs removed, the hazard ratio for disease-related death (adjusted for T stage, R status, grade, receipt of neoadjuvant and adjuvant therapy, and institution) significantly decreased as the number of LNs removed increased.
Conclusions: The number of LNs removed during gastrectomy for adenocarcinoma appears itself to have prognostic implications for long-term survival.
Copyright © 2015 American College of Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Jemal A, Bray F, Center MM, et al. Global Cancer Statistics. CA Cancer J Clin. 2011;61:69–90. - PubMed
-
- Maruyama K, Okabayashi K, Kinoshita T. Progress in gastric cancer surgery in Japan and its limits of radicality. World J Surg. 1987;11:418–425. - PubMed
-
- Cuschieri A, Fayers P, Fielding J, et al. Postoperative morbidity and mortality after D1 and D2 resections for gastric cancer: preliminary results of the MRC randomised controlled surgical trial. The Surgical Cooperative Group. Lancet. 1996;347:995–999. - PubMed
-
- Bonenkamp JJ, Hermans J, Sasako M, et al. Extended lymph-node dissection for gastric cancer. N Engl J Med. 1999;340:908–914. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
