

Extended Intervals after Neoadjuvant Therapy in Locally Advanced Rectal Cancer: The Key to Improved Tumor Response and Potential Organ Preservation
- PMID: 26206642
- PMCID: PMC5014360
- DOI: 10.1016/j.jamcollsurg.2015.04.010
Extended Intervals after Neoadjuvant Therapy in Locally Advanced Rectal Cancer: The Key to Improved Tumor Response and Potential Organ Preservation
Abstract
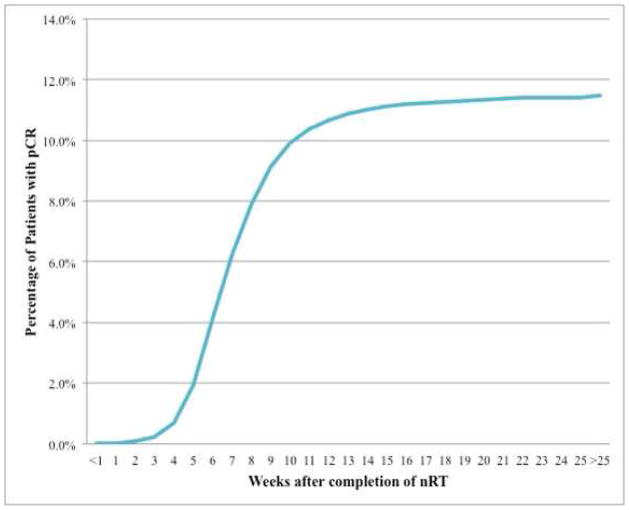
Background: Many rectal cancer patients experience tumor downstaging and some are found to achieve a pathologic complete response (pCR) after neoadjuvant chemoradiotherapy (nCRT). Previous data suggest that there is an association between the time interval from nCRT completion to surgery and tumor response rates, including pCR. However, these studies have been primarily from single institutions with small sample sizes. The aim of this study was to examine the relationship between a longer interval after nCRT and pCR in a nationally representative cohort of rectal cancer patients.
Study design: Clinical stage II to III rectal cancer patients undergoing nCRT with a documented surgical resection were selected from the 2006 to 2011 National Cancer Data Base. Multivariable logistic regression analysis was used to assess the association between the nCRT-surgery interval time (<6 weeks, 6 to 8 weeks, >8 weeks) and the odds of pCR. The relationship between nCRT-surgery interval, surgical morbidity, and tumor downstaging was also examined.
Results: Overall, 17,255 patients met the inclusion criteria. An nCRT-surgery interval time >8 weeks was associated with higher odds of pCR (odds ratio [OR] 1.12, 95% CI 1.01 to 1.25) and tumor downstaging (OR 1.11, 95% CI 1.02 to 1.25). The longer time delay was also associated with lower odds of 30-day readmission (OR 0.82, 95% CI 0.70 to 0.92).
Conclusions: An nCRT-surgery interval time >8 weeks results in increased odds of pCR, with no evidence of associated increased surgical complications compared with an interval of 6 to 8 weeks. These data support implementation of a lengthened interval after nCRT to optimize the chances of pCR and perhaps add to the possibility of ultimate organ preservation (nonoperative management).
Copyright © 2015 American College of Surgeons. Published by Elsevier Inc. All rights reserved.
Figures

References
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin. 2013 Jan;63(1):11–30. - PubMed
-
- Fleming FJ, Pahlman L, Monson JR. Neoadjuvant therapy in rectal cancer. Dis Colon Rectum. 2011 Jul;54(7):901–12. - PubMed
-
- Ricciardi R, Roberts PL, Read TE, et al. Who performs proctectomy for rectal cancer in the United States? Dis Colon Rectum. 2011 Oct;54(10):1210–5. - PubMed
-
- Benson AB, 3rd, Bekaii-Saab T, Chan E, et al. Rectal cancer. J Natl Compr Canc Netw. 2012 Dec 1;10(12):1528–64. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
