

Goal-Directed Fluid Therapy Using Stroke Volume Variation for Resuscitation after Low Central Venous Pressure-Assisted Liver Resection: A Randomized Clinical Trial
- PMID: 26206652
- PMCID: PMC4926263
- DOI: 10.1016/j.jamcollsurg.2015.03.050
Goal-Directed Fluid Therapy Using Stroke Volume Variation for Resuscitation after Low Central Venous Pressure-Assisted Liver Resection: A Randomized Clinical Trial
Abstract
Background: The optimal perioperative fluid resuscitation strategy for liver resections remains undefined. Goal-directed therapy (GDT) embodies a number of physiologic strategies to achieve an ideal fluid balance and avoid the consequences of over- or under-resuscitation.
Study design: In a prospective randomized trial, patients undergoing liver resection were randomized to GDT using stroke volume variation as an end point or to standard perioperative resuscitation. Primary outcomes measure was 30-day morbidity.
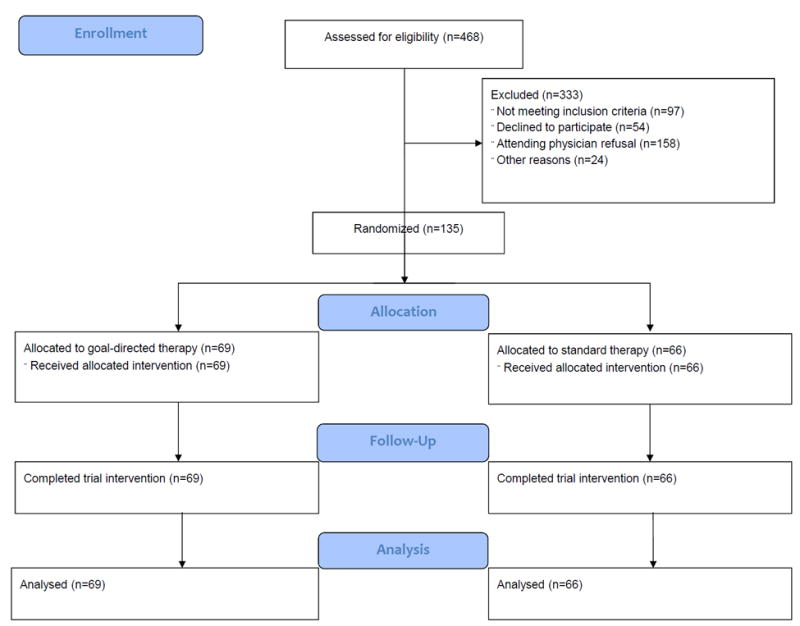
Results: Between 2012 and 2014, one hundred and thirty-five patients were randomized (GDT: n = 69; standard perioperative resuscitation: n = 66). Median age was 57 years and 56% were male. Metastatic disease comprised 81% of patients. Overall (35% GDT vs 36% standard perioperative resuscitation; p = 0.86) and grade 3 morbidity (28% GDT vs 18% standard perioperative resuscitation; p = 0.22) were equivalent. Patients in the GDT arm received less intraoperative fluid (mean 2.0 L GDT vs 2.9 L standard perioperative resuscitation; p < 0.001). Perioperative transfusions were required in 4% (6% GDT vs 2% standard perioperative resuscitation; p = 0.37) and boluses in the postanesthesia care unit were administered to 24% (29% GDT vs 20% standard perioperative resuscitation; p = 0.23). Mortality rate was 1% (2 of 135 patients; both in GDT). On multivariable analysis, male sex, age, combined procedures, higher intraoperative fluid volume, and fluid boluses in the postanesthesia care unit were associated with higher 30-day morbidity.
Conclusions: Stroke volume variation-guided GDT is safe in patients undergoing liver resection and led to less intraoperative fluid. Although the incidence of postoperative complications was similar in both arms, lower intraoperative resuscitation volume was independently associated with decreased postoperative morbidity in the entire cohort. Future studies should target extensive resections and identify patients receiving large resuscitation volumes, as this population is more likely to benefit from this technique.
Trial registration: ClinicalTrials.gov NCT01596283.
Copyright © 2015 American College of Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
What Is a Good Perioperative Intravenous Fluid Therapy in Liver Surgery?J Am Coll Surg. 2016 Jan;222(1):97. doi: 10.1016/j.jamcollsurg.2015.09.017. J Am Coll Surg. 2016. PMID: 26721751 No abstract available.
-
Optimal Fluid Resuscitation after Liver Resection: An Evolving Concept: In Reply to Geerts and colleagues.J Am Coll Surg. 2016 Jan;222(1):97-8. doi: 10.1016/j.jamcollsurg.2015.09.018. J Am Coll Surg. 2016. PMID: 26721752 No abstract available.
References
-
- Pearse RM, Harrison DA, MacDonald N, et al. Effect of a perioperative, cardiac output-guided hemodynamic therapy algorithm on outcomes following major gastrointestinal surgery: a randomized clinical trial and systematic review. JAMA. 2014;311:2181–2190. - PubMed
-
- Bundgaard-Nielsen M, Secher NH, Kehlet H. ‘Liberal’ vs. ‘restrictive’ perioperative fluid therapy--a critical assessment of the evidence. Acta Anaesthesiol Scand. 2009;53:843–851. - PubMed
-
- Della Rocca G, Pompei L. Goal-directed therapy in anesthesia: any clinical impact or just a fashion? Minerva Anestesiol. 2011 - PubMed
-
- Peng K, Li J, Cheng H, Ji FH. Goal-directed fluid therapy based on stroke volume variations improves fluid management and gastrointestinal perfusion in patients undergoing major orthopedic surgery. Medical principles and practice : international journal of the Kuwait University, Health Science Centre. 2014 - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
