

A New Targeted Model of Experimental Autoimmune Encephalomyelitis in the Common Marmoset
- PMID: 26207848
- PMCID: PMC8029260
- DOI: 10.1111/bpa.12292
A New Targeted Model of Experimental Autoimmune Encephalomyelitis in the Common Marmoset
Abstract
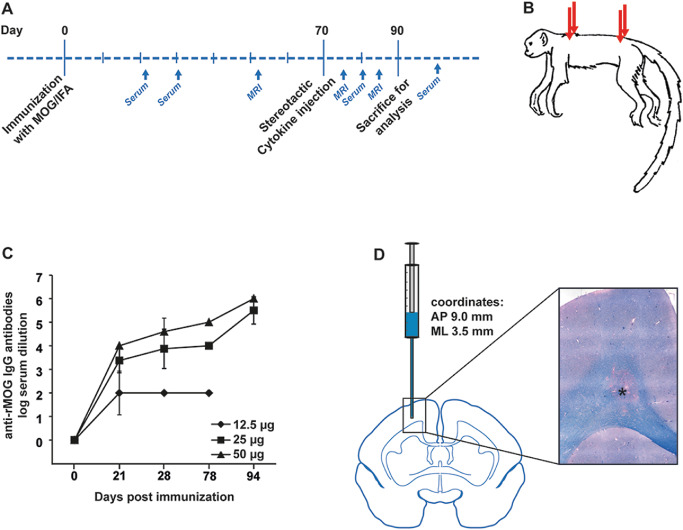
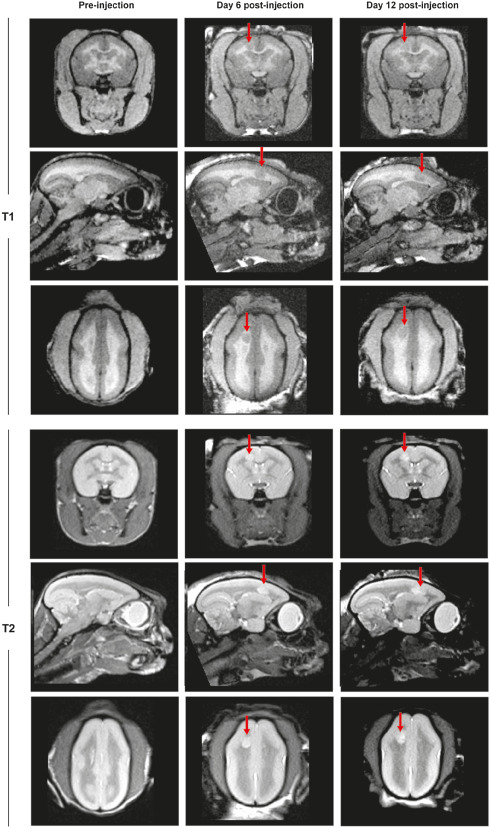
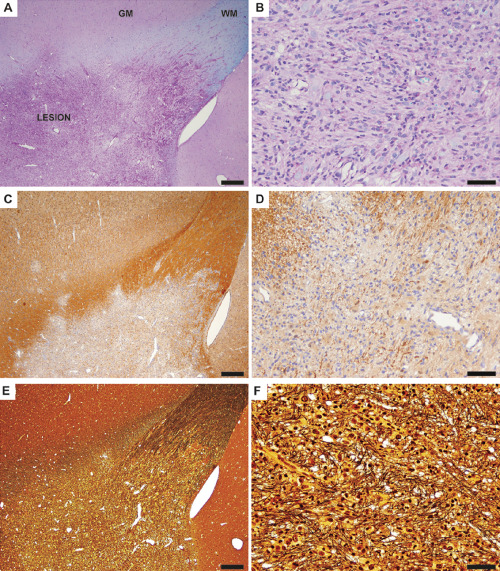
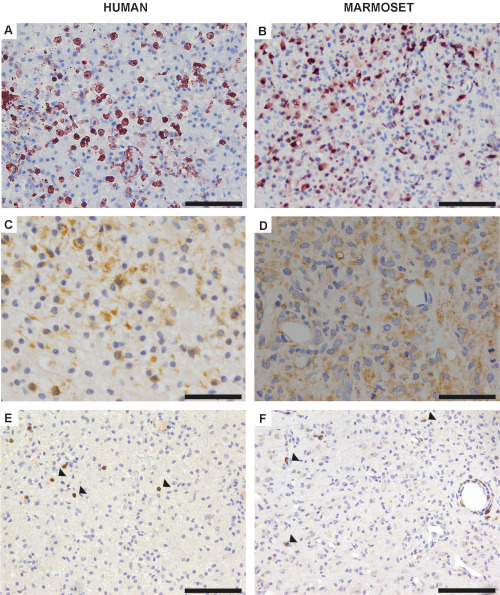
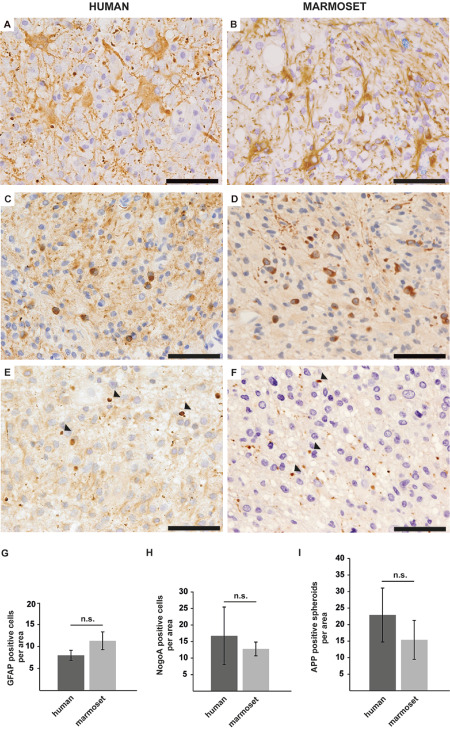
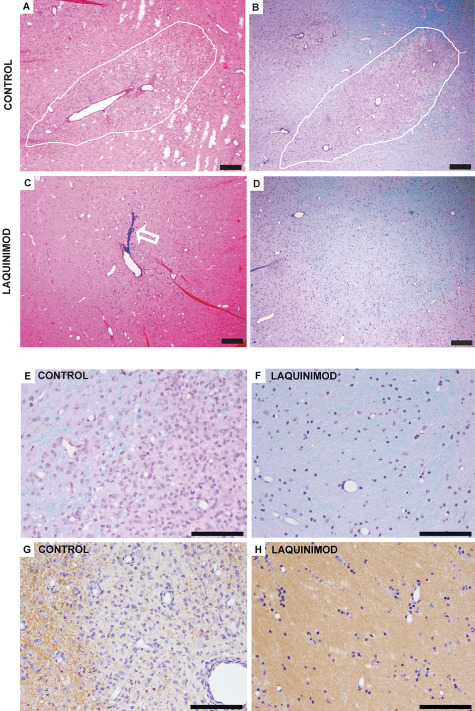
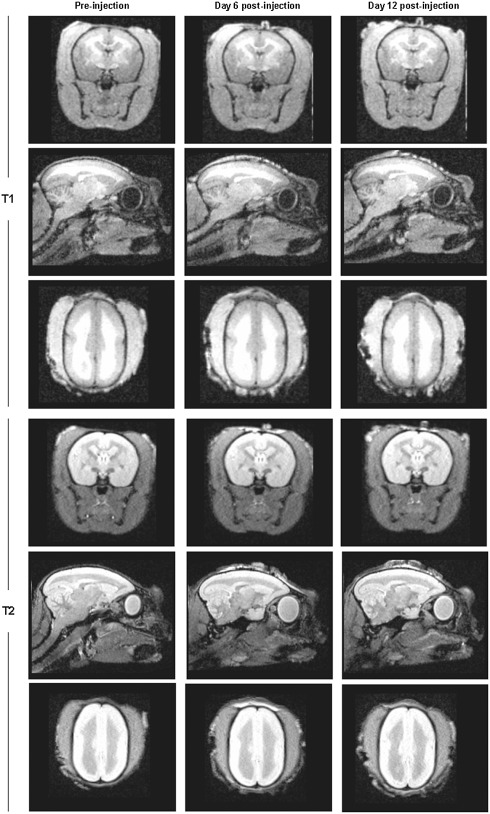
Multiple sclerosis (MS) is the most common cause for sustained disability in young adults, yet treatment options remain very limited. Although numerous therapeutic approaches have been effective in rodent models of experimental autoimmune encephalomyelitis (EAE), only few proved to be beneficial in patients with MS. Hence, there is a strong need for more predictive animal models. Within the past decade, EAE in the common marmoset evolved as a potent, alternative model for MS, with immunological and pathological features resembling more closely the human disease. However, an often very rapid and severe disease course hampers its implementation for systematic testing of new treatment strategies. We here developed a new focal model of EAE in the common marmoset, induced by myelin oligodendrocyte glycoprotein (MOG) immunization and stereotactic injections of proinflammatory cytokines. At the injection site of cytokines, confluent inflammatory demyelinating lesions developed that strongly resembled human MS lesions. In a proof-of-principle treatment study with the immunomodulatory compound laquinimod, we demonstrate that targeted EAE in marmosets provides a promising and valid tool for preclinical experimental treatment trials in MS research.
Keywords: common marmoset; demyelination; experimental autoimmune encephalomyelitis; immunomodulation; laquinimod; multiple sclerosis.
© 2015 International Society of Neuropathology.
Conflict of interest statement
The authors have nothing to disclose and no conflict of interest to report.
Figures
References
-
- Boretius S, Schmelting B, Watanabe T, Merkler D, Tammer R, Czéh B et al (2006) Monitoring of EAE onset and progression in the common marmoset monkey by sequential high‐resolution 3D MRI. NMR Biomed 19:41–49. - PubMed
-
- Brück W, Vollmer T (2013) Multiple sclerosis: oral laquinimod for MS—bringing the brain into focus. Nat Rev Neurol 9:664–665. - PubMed
-
- Brück W, Porada P, Poser S, Rieckmann P, Hanefeld F, Kretzschmar HA, Lassmann H (1995) Monocyte/macrophage differentiation in early multiple sclerosis lesions. Ann Neurol 38:788–796. - PubMed
-
- Gardner C, Magliozzi R, Durrenberger PF, Howell OW, Rundle J, Reynolds R (2013) Cortical grey matter demyelination can be induced by elevated pro‐inflammatory cytokines in the subarachnoid space of MOG‐immunized rats. Brain 136:3596–3608. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
