

Hyperuricemia and Progression of CKD in Children and Adolescents: The Chronic Kidney Disease in Children (CKiD) Cohort Study
- PMID: 26209544
- PMCID: PMC4658318
- DOI: 10.1053/j.ajkd.2015.06.015
Hyperuricemia and Progression of CKD in Children and Adolescents: The Chronic Kidney Disease in Children (CKiD) Cohort Study
Abstract
Background: Hyperuricemia is associated with essential hypertension in children. No previous studies have evaluated the effect of hyperuricemia on progression of chronic kidney disease (CKD) in children.
Study design: Prospective observational cohort study.
Setting & participants: Children and adolescents (n=678 cross-sectional; n=627 longitudinal) with a median age of 12.3 (IQR, 8.6-15.6) years enrolled at 52 North American sites of the CKiD (CKD in Children) Study.
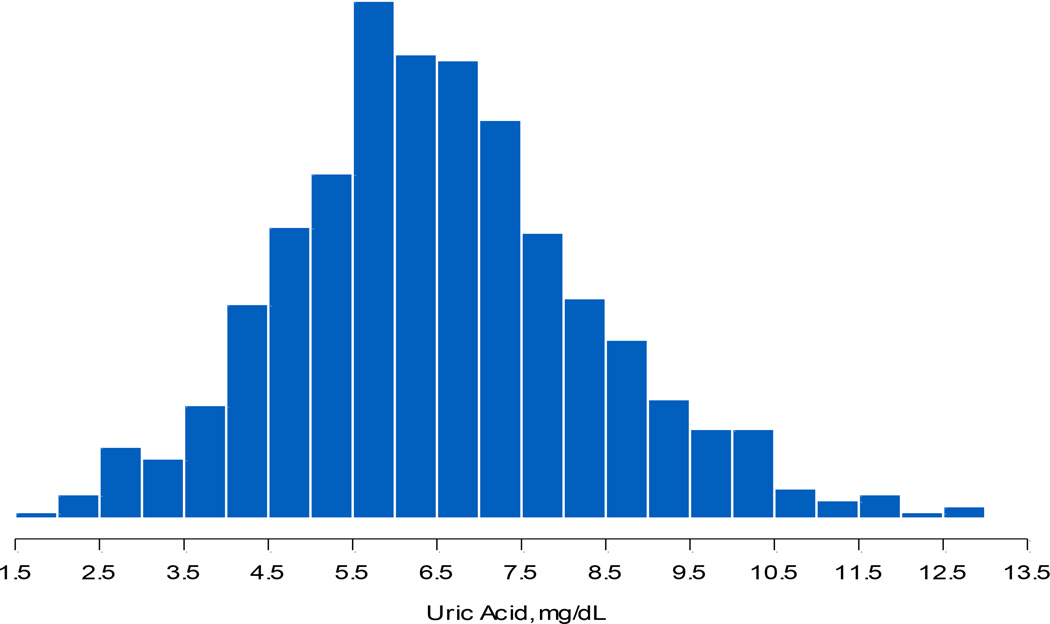
Predictor: Serum uric acid level (<5.5, 5.5-7.5, and >7.5mg/dL).
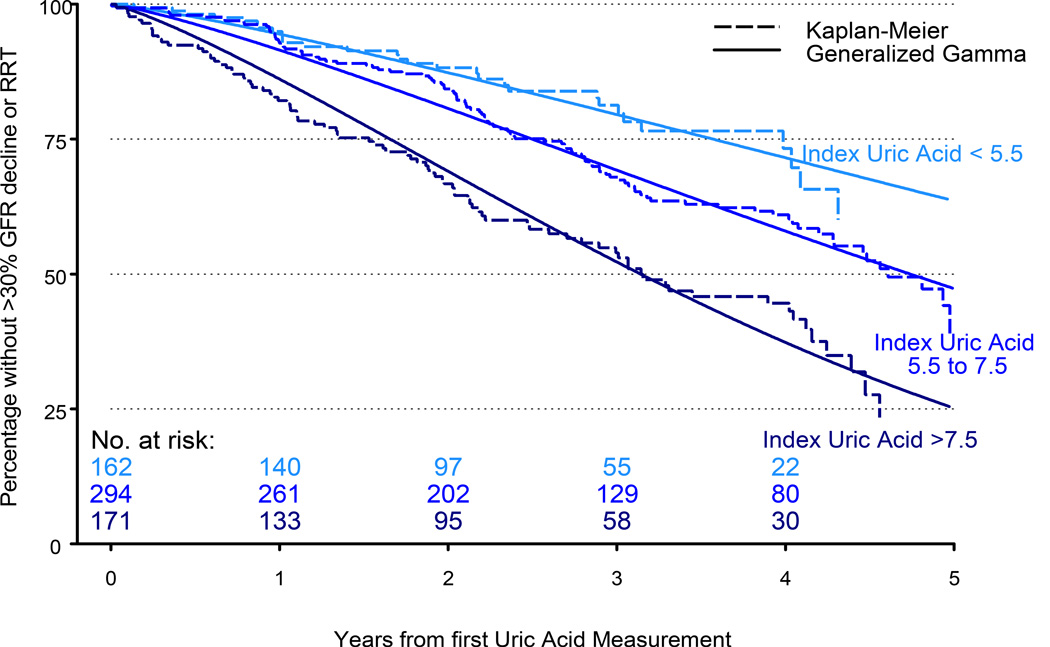
Outcomes: Composite end point of either >30% decline in glomerular filtration rate (GFR) or initiation of renal replacement therapy.
Measurements: Age, sex, race, blood pressure status, GFR, CKD cause, urine protein-creatinine ratio (<0.5, 0.5-<2.0, and ≥2.0mg/mg), age- and sex-specific body mass index > 95th percentile, use of diuretics, and serum uric acid level.
Results: Older age, male sex, lower GFR, and body mass index > 95th percentile were associated with higher uric acid levels. 162, 294, and 171 participants had initial uric acid levels < 5.5, 5.5 to 7.5, or >7.5 mg/dL, respectively. We observed 225 instances of the composite end point over 5 years. In a multivariable parametric time-to-event analysis, compared with participants with initial uric acid levels < 5.5mg/dL, those with uric acid levels of 5.5 to 7.5 or >7.5mg/dL had 17% shorter (relative time, 0.83; 95% CI, 0.62-1.11) or 38% shorter (relative time, 0.62; 95% CI, 0.45-0.85) times to event, respectively. Hypertension, lower GFR, glomerular CKD cause, and elevated urine protein-creatinine ratio were also associated with faster times to the composite end point.
Limitations: The study lacked sufficient data to examine how use of specific medications might influence serum uric acid levels and CKD progression.
Conclusions: Hyperuricemia is a previously undescribed independent risk factor for faster progression of CKD in children and adolescents. It is possible that treatment of children and adolescents with CKD with urate-lowering therapy could slow disease progression.
Keywords: CKD progression; CKiD (Chronic Kidney Disease in Children); Uric acid; adolescents; children; chronic kidney disease (CKD); disease trajectory; end-stage renal disease (ESRD); glomerular filtration rate (GFR); hyperuricemia; pediatric kidney disease; renal function decline; renal replacement therapy (RRT); risk factor; urate.
Copyright © 2015 National Kidney Foundation, Inc. All rights reserved.
Figures
References
-
- Feig DI. Serum uric acid and the risk of hypertension and chronic kidney disease. Curr Opin Rheumatol. 2014;26(2):76–185. - PubMed
-
- Dawson J, Jeemon P, Hetherington L, et al. Serum uric acid level, longitudinal blood pressure, renal function, and long-term mortality in treated hypertensive patients. Hypertension. 2013;62(1):105–111. - PubMed
-
- Krishnan E, Akhras KS, Sharma H, et al. Serum Urate and Incidence of Kidney Disease Among Veterans with Gout. J Rheumatol. 2013;40(7):1166–1172. - PubMed
-
- Ohta Y, Tsuchihashi T, Kiyohara K, Oniki H. Increased uric acid promotes decline of the renal function in hypertensive patients: a 10-year observational study. Intern Med. 2012;52(13):467–1472. - PubMed
-
- Alper AB, Chen W, Yau L, Srinivasan SR, Berenson GS, Hamm LL. Childhood Uric Acid Predicts Adult Blood Pressure The Bogalusa Heart Study. Hypertension. 2005;45(1):34–38. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
