

Survival in systemic sclerosis-pulmonary arterial hypertension by serum autoantibody status in the Pulmonary Hypertension Assessment and Recognition of Outcomes in Scleroderma (PHAROS) Registry
- PMID: 26210782
- PMCID: PMC4656087
- DOI: 10.1016/j.semarthrit.2015.06.011
Survival in systemic sclerosis-pulmonary arterial hypertension by serum autoantibody status in the Pulmonary Hypertension Assessment and Recognition of Outcomes in Scleroderma (PHAROS) Registry
Abstract
Objective: To determine the association between serum autoantibodies and survival in patients with incident systemic sclerosis (SSc)-pulmonary arterial hypertension (PAH) enrolled in the Pulmonary Hypertension Assessment and Recognition of Outcomes in Scleroderma (PHAROS) Registry.
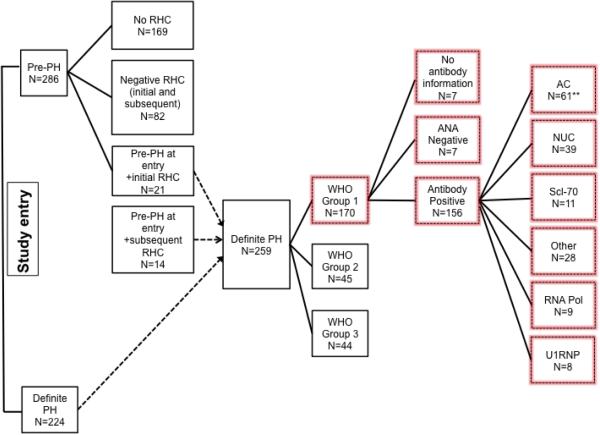
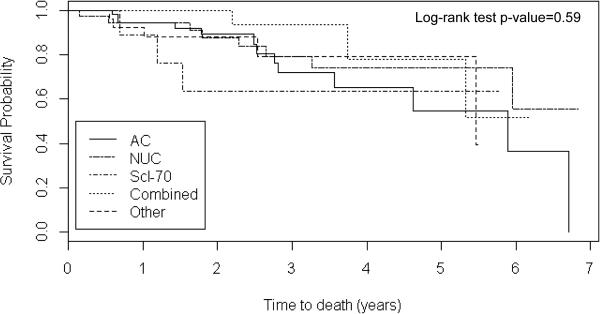
Methods: Patients with definite PAH diagnosed by right heart catheterization within 6 months of registry enrollment were studied. Serum autoantibodies were assayed at each participating institution's clinical laboratory. Mortality data were collected from electronic medical records and/or the Social Security Death Index. Kaplan-Meier survival estimates were reported for five autoantibody groups (anticentromere/AC, nucleolar ANA/NUC, anti-topoisomerase/Scl-70, overlapping or non-specific autoantibodies/other, and a combined group with similar survival consisting of RNA polymerase III, U1RNP, and autoantibody-negative patients). Cox proportional hazards models permitted examination of the association between autoantibody groups and overall survival, controlling for age, sex, race, and SSc disease duration.
Results: In all, 162 subjects had PAH, and serum autoantibody and survival information; 60 (37%) had AC, 39 (24%) NUC, 11 (7%) Scl-70, 28 (17%) had other, 9 (6%) RNA pol, 8 (5%) U1RNP autoantibodies, and 7 (4%) had negative antibodies; 32 (20%) subjects died over a median follow-up time of 2.1 years (range: 0.01-6.8); 1- and 3-year survival estimates were, respectively, 94% and 78% for AC, 94% and 72% for NUC, 89% and 63% for Scl-70, 92% and 79% for the other group, and 100% and 93% for the combined group. Unadjusted and adjusted hazard ratios revealed no statistically significant association between risk of death and autoantibodies.
Conclusion: Anticentromere and NUC autoantibodies are prevalent in SSc-PAH patients. An association between serum autoantibodies and survival in patients with SSc-PAH was not identified in the PHAROS cohort.
Keywords: Mortality; Pulmonary arterial hypertension; Pulmonary hypertension; Risk factors; Scleroderma; Serum autoantibody; Systemic sclerosis.
Copyright © 2015 Elsevier Inc. All rights reserved.
Figures
References
-
- Nihtyanova SI, Schreiber BE, Ong VH, Rosenberg D, Moinzadeh P, Coghlan JG, et al. Prediction of pulmonary complications and long term survival in systemic sclerosis. Arthritis & rheumatology (Hoboken, NJ) 2014 - PubMed
-
- Steen VD. Autoantibodies in systemic sclerosis. Semin Arthritis Rheum. 2005;35(1):1–35. - PubMed
-
- Doering K, Rosen A. Autoantibodies in Pathogenesis. In: Varga J, Denton C, Wigley F, editors. Scleroderma: From Pathogenesis to Comprehensive Management. Springer; New York, Dordrecht, Heidelberg, London: 2012. pp. 199–208.
-
- Galie N, Hoeper MM, Humbert M, Torbicki A, Vachiery JL, Barbera JA, et al. Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Respir J. 2009;34(6):6–1219. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
