

The open abdomen, indications, management and definitive closure
- PMID: 26213565
- PMCID: PMC4515003
- DOI: 10.1186/s13017-015-0026-5
The open abdomen, indications, management and definitive closure
Abstract
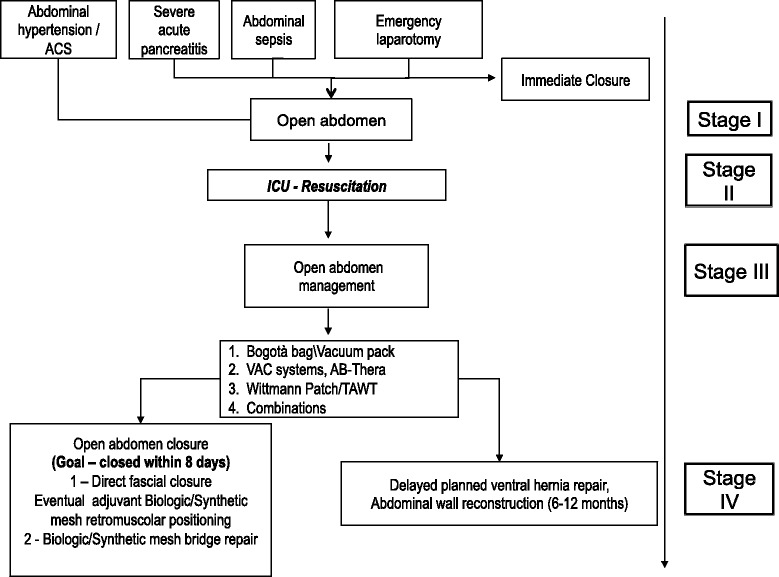
The indications for Open Abdomen (OA) are generally all those situations in which is ongoing the development an intra-abdominal hypertension condition (IAH), in order to prevent the development of abdominal compartmental syndrome (ACS). In fact all those involved in care of a critically ill patient should in the first instance think how to prevent IAH and ACS. In case of ACS goal directed therapy to achieve early opening and early closure is the key: paradigm of closure shifts to combination of therapies including negative pressure wound therapy and dynamic closure, in order to reduce complications and avoid incisional hernia. There have been huge studies and progress in survival of critically ill trauma and septic surgical patients: this in part has been through the great work of pioneers, scientific societies and their guidelines; however future studies and continued innovation are needed to better understand optimal treatment strategies and to define more clearly the indications, because OA by itself is still a morbid procedure.
Keywords: Closure; Management; Open abdomen; Pancreatitis; Peritonitis; Trauma.
Figures


Similar articles
-
Prophylactic open abdomen in patients with postoperative intra-abdominal hypertension.Crit Care. 2010;14(1):111. doi: 10.1186/cc8207. Epub 2010 Feb 4. Crit Care. 2010. PMID: 20156323 Free PMC article.
-
IROA: the International Register of Open Abdomen.: An international effort to better understand the open abdomen: call for participants.World J Emerg Surg. 2015 Aug 16;10:37. doi: 10.1186/s13017-015-0029-2. eCollection 2015. World J Emerg Surg. 2015. PMID: 26279673 Free PMC article.
-
Early Initiation of a Standardized Open Abdomen Treatment With Vacuum Assisted Mesh-Mediated Fascial Traction Achieves Best Results.Front Surg. 2021 Feb 9;7:606539. doi: 10.3389/fsurg.2020.606539. eCollection 2020. Front Surg. 2021. PMID: 33634162 Free PMC article.
-
Intra-abdominal hypertension and the abdominal compartment syndrome: updated consensus definitions and clinical practice guidelines from the World Society of the Abdominal Compartment Syndrome.Intensive Care Med. 2013 Jul;39(7):1190-206. doi: 10.1007/s00134-013-2906-z. Epub 2013 May 15. Intensive Care Med. 2013. PMID: 23673399 Free PMC article.
-
The open abdomen in trauma, acute care, and vascular and endovascular surgery: comprehensive, expert, narrative review.BJS Open. 2023 Sep 5;7(5):zrad084. doi: 10.1093/bjsopen/zrad084. BJS Open. 2023. PMID: 37882630 Free PMC article. Review.
Cited by
-
Double-Breasted Anterior Rectus Sheath Turnover Flap.Cureus. 2023 Nov 23;15(11):e49302. doi: 10.7759/cureus.49302. eCollection 2023 Nov. Cureus. 2023. PMID: 38957194 Free PMC article.
-
Open Abdomen Management and Candida Infections: A Very Likely Link.Gastroenterol Res Pract. 2017;2017:5187620. doi: 10.1155/2017/5187620. Epub 2017 Dec 7. Gastroenterol Res Pract. 2017. PMID: 29362562 Free PMC article.
-
Characterization of hypoalbuminemia following temporary abdominal closure.J Trauma Acute Care Surg. 2017 Oct;83(4):650-656. doi: 10.1097/TA.0000000000001553. J Trauma Acute Care Surg. 2017. PMID: 28837537 Free PMC article.
-
Retrospective validation of parkland grading scale in a Latin-American high-volume center.Surg Endosc. 2023 Jul;37(7):5190-5195. doi: 10.1007/s00464-023-09946-3. Epub 2023 Mar 22. Surg Endosc. 2023. PMID: 36947228
-
Novel method for delayed primary closure and incisional hernia prevention in open abdomen: COmbined and MOdified Definitive Abdominal wall closure (COMODA).Hernia. 2020 Apr;24(2):395-401. doi: 10.1007/s10029-019-01948-2. Epub 2019 Apr 9. Hernia. 2020. PMID: 30968285 Clinical Trial.
References
-
- Ogilvie WH. The late complications of abdominal war wounds. Lancet. 1940;2:253–6. doi: 10.1016/S0140-6736(01)08769-4. - DOI
LinkOut - more resources
Full Text Sources
Other Literature Sources
