

Doctors or mid-level providers for abortion
- PMID: 26214844
- PMCID: PMC9188302
- DOI: 10.1002/14651858.CD011242.pub2
Doctors or mid-level providers for abortion
Abstract
Background: The World Health Organization recommends that abortion can be provided at the lowest level of the healthcare system. Training mid-level providers, such as midwives, nurses and other non-physician providers, to conduct first trimester aspiration abortions and manage medical abortions has been proposed as a way to increase women's access to safe abortion procedures.
Objectives: To assess the safety and effectiveness of abortion procedures administered by mid-level providers compared to doctors.
Search methods: We searched the CENTRAL Issue 7, MEDLINE and POPLINE databases for comparative studies of doctor and mid-level providers of abortion services. We searched for studies published in any language from January 1980 until 15 August 2014.
Selection criteria: Randomised controlled trials (RCTs) (clustered or not clustered), prospective cohort studies or observational studies that compared the safety or effectiveness (or both) of any type of first trimester abortion procedure, administered by any type of mid-level provider or doctors, were eligible for inclusion in the review.
Data collection and analysis: Two independent review authors screened abstracts for eligibility and double-extracted data from the included studies using a pre-tested form. We meta-analysed primary outcome data using both fixed-effect and random-effects models to obtain pooled risk ratios (RR) with 95% confidence intervals (CIs). We carried out separate analyses by study design (RCT or cohort) and type of abortion procedure (medical versus surgical).
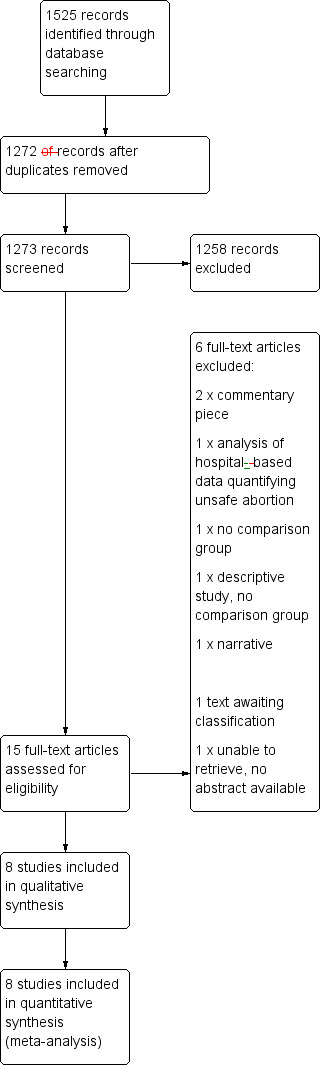
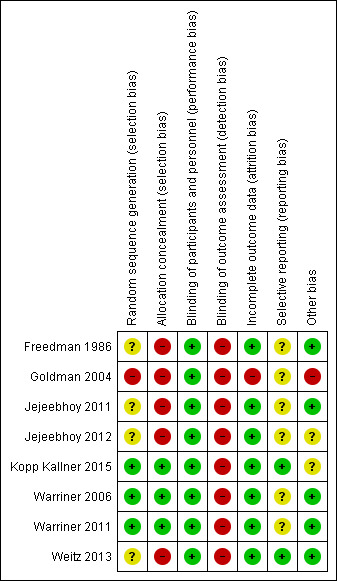
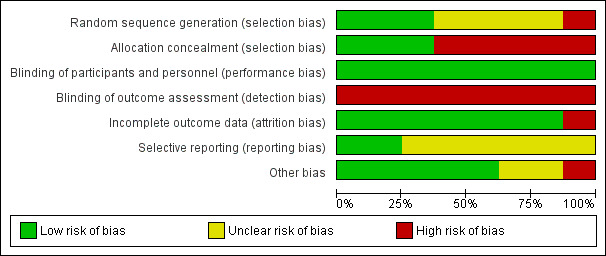
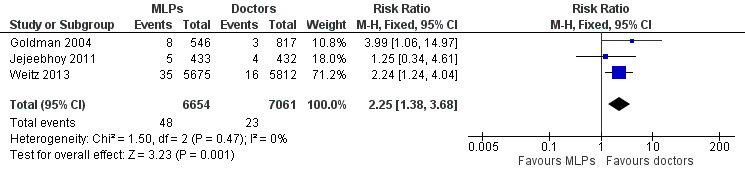
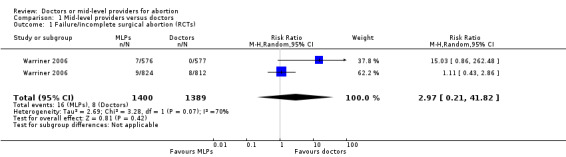
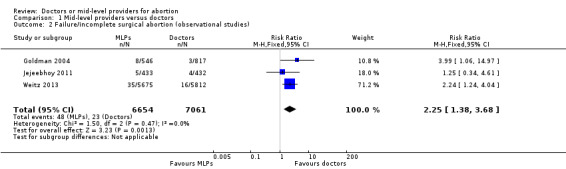
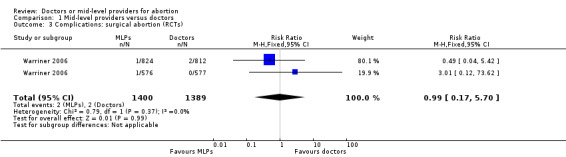
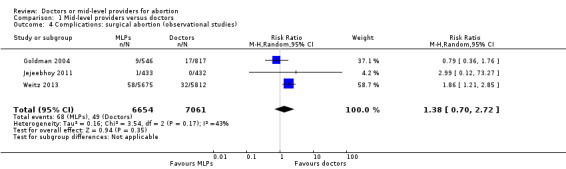
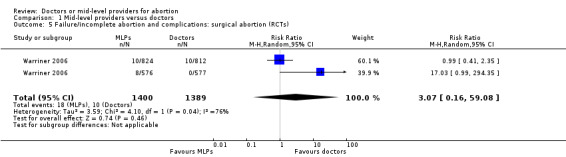
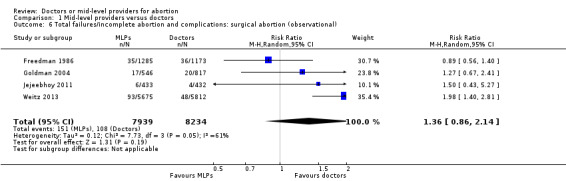
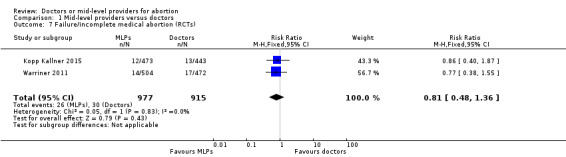
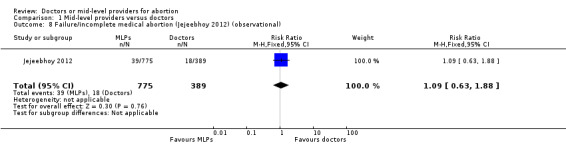
Main results: Eight studies involving 22,018 participants met our eligibility criteria. Five studies (n = 18,962) assessed the safety and effectiveness of surgical abortion procedures administered by mid-level providers compared to doctors. Three studies (n = 3056) assessed the safety and effectiveness of medical abortion procedures. The surgical abortion studies (one RCT and four cohort studies) were carried out in the United States, India, South Africa and Vietnam. The medical abortion studies (two RCTs and one cohort study) were carried out in India, Sweden and Nepal. The studies included women with gestational ages up to 14 weeks for surgical abortion and nine weeks for medical abortion.Risk of selection bias was considered to be low in the three RCTs, unclear in four observational studies and high in one observational study. Concealment bias was considered to be low in the three RCTs and high in all five observational studies. Although none of the eight studies performed blinding of the participants to the provider type, we considered the performance bias to be low as this is part of the intervention. Detection bias was considered to be high in all eight studies as none of the eight studies preformed blinding of the outcome assessment. Attrition bias was low in seven studies and high in one, with over 20% attrition. We considered six studies to have unclear risk of selective reporting bias as their protocols had not been published. The remaining two studies had published their protocols. Few other sources of bias were found.Based on an analysis of three cohort studies, the risk of surgical abortion failure was significantly higher when provided by mid-level providers than when procedures were administered by doctors (RR 2.25, 95% CI 1.38 to 3.68), however the quality of evidence for this outcome was deemed to be very low. For surgical abortion procedures, we found no significant differences in the risk of complications between mid-level providers and doctors (RR 0.99, 95% CI 0.17 to 5.70 from RCTs; RR 1.38, 95% CI 0.70 to 2.72 from observational studies). When we combined the data for failure and complications for surgical abortion we found no significant differences between mid-level providers and doctors in both the observational study analysis (RR 1.36, 95% CI 0.86 to 2.14) and the RCT analysis (RR 3.07, 95% CI 0.16 to 59.08). The quality of evidence of the outcome for RCT studies was considered to be low and for observational studies very low. For medical abortion procedures the risk of failure was not different for mid-level providers or doctors (RR 0.81, 95% CI 0.48 to 1.36 from RCTs; RR 1.09, 95% CI 0.63 to 1.88 from observational studies). The quality of evidence of this outcome for the RCT analysis was considered to be high, although the quality of evidence of the observational studies was considered to be very low. There were no complications reported in the three medical abortion studies.
Authors' conclusions: There was no statistically significant difference in the risk of failure for medical abortions performed by mid-level providers compared with doctors. Observational data indicate that there may be a higher risk of abortion failure for surgical abortion procedures administered by mid-level providers, but the number of studies is small and more robust data from controlled trials are needed. There were no statistically significant differences in the risk of complications for first trimester surgical abortions performed by mid-level providers compared with doctors.
Conflict of interest statement
Sharmani Barnard: nothing to declare. Caron Kim: nothing to declare. Min Hae Park: nothing to declare. Thoai D. Ngo: nothing to declare.
Figures
Update of
References
References to studies included in this review
Freedman 1986 {published data only}
Goldman 2004 {published data only}
Jejeebhoy 2011 {published data only}
-
- Jejeebhoy SJ, Kalyanwalaa S, Zaviera AJF, Kumara R, Mundleb S, Tankc J, et al. Can nurses perform manual vacuum aspiration (MVA) as safely and effectively as physicians? Evidence from India. Contraception 2011;84:615–21. - PubMed
Jejeebhoy 2012 {published data only}
-
- Jejeebhoy SJ, Kalyanwalaa S, Zaviera AJF, Kumara R, Mundleb S, Tankc J, et al. Feasibility of expanding the medication abortion provider base in India to include ayurvedic physicians and nurses. International Perspectives on Sexual and Reproductive Health 2012;38(3):133‐42. - PubMed
Kopp Kallner 2015 {published data only}
-
- Kopp Kallner H, Gomperts R, Salomonsson E, Johansson M, Marions L, Gemzell‐Danielsson K. The efficacy, safety and acceptability of medical termination of pregnancy provided by standard care by doctors or by nurse midwives: a randomised controlled equivalence trial. BJOG 2015 ; 122 ( 4 ):510‐7. [DOI: 10.1111/1471-0528.12982] - DOI - PubMed
Warriner 2006 {published data only}
-
- Warriner IK, Meirik O, Hoffman M, Morroni C, Harries J, My Huong NT, et al. Rates of complication in first‐trimester manual vacuum aspiration abortion done by doctors and mid‐level providers in South Africa and Vietnam: a randomised controlled equivalence trial. Lancet 2006;368:1965‐72. [DOI: 10.1016/S0140-6736(06)69742-0] - DOI - PubMed
Warriner 2011 {published data only}
-
- Warriner IK, Wang D, My Huong NT, Thapa K, Tamang A, Shah I, et al. Can midlevel health‐care providers administer early medical abortion as safely and effectively as doctors? A randomised controlled equivalence trial in Nepal. Lancet 2011;377:1155–61. - PubMed
Weitz 2013 {published data only}
References to studies excluded from this review
Donovan 1992 {published data only}
-
- Donovan P. Vermont physician assistants perform abortions, train residents. Family Planning Perspectives 1992;24(5):225. - PubMed
Igberase 2008 {published data only}
-
- Igberase GO, Ebeigbe PN. Exploring the pattern of complications of induced abortion in a rural mission tertiary hospital in the Niger Delta, Nigeria. Tropical Doctor 2008;38(3):146‐8. - PubMed
IPPF 2001 {published data only}
-
- International Planned Parenthood Federation (IPPF), South Asia Region. Expanding the role of traditional birth attendants: experiences from South Asia. IPPF, South Asia Region: London, England 2001:44.
Neustatter 1980 {published data only}
-
- Neustatter PL. Participation of nurses in abortions . Lancet 1980;2(8205):1199‐200. - PubMed
Shaikh 2010 {published data only}
-
- Shaikh Z, Abbassi RM, Rizwan N, Abbasi S. Morbidity and mortality due to unsafe abortion in Pakistan. International Journal of Gynaecology and Obstetrics 2010;110(1):47‐9. - PubMed
Shamash 2002 {published data only}
-
- Shamash J. Abortion: is it a step too far for nurses?. Nursing Times 2002;98(28):12. - PubMed
References to studies awaiting assessment
Additional references
Acharya 2014
-
- Acharya R, Kalyanwala S. Physicians' and non‐physicians' views about provision of medical abortion by nurses and AYUSH physicians in Maharashtra and Bihar, India. Reproductive Health Matters 2014;Suppl(43):1‐11. - PubMed
Berer 2009
Brown 2011
-
- Brown A, Cometto G, Cumbi A, Pinho H, Kamwendo F, Lehmann U, et al. Mid‐level health providers: a promising resource to achieve the health Millennium Development Goals. Revista P eruana de M edicina Experimental y S alud Pública 2011;28(2):308‐15. - PubMed
Chong 2006
-
- Chong YS, Mattar CN. Midlevel providers: a safe solution for unsafe abortion. Lancet 2006;368(9551):1939‐40. - PubMed
Higgins 2011
-
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
IPAS 2002
-
- Ipas, IHCAR. Deciding women's lives are worth saving: expanding the role of midlevel providers in safe abortion care. Ipas. Chapel Hill, 2002. [1‐882220‐33‐1]
Jones 2000
-
- Jones RK, Henshaw SK. Mifepristone for early medical abortion: experiences in France, Great Britain and Sweden. Perspectives on Sexual and Reproductive Health 2000;34(3):154‐61. - PubMed
Kulier 2009
Kulier 2011
Long 2001
-
- Long C, Ren N. Abortion in Cambodia: country report. Expanding Access: Midlevel Providers in Menstrual Regulation and Elective Abortion Care; 2001 Dec 3‐6; South Africa. 2001.
Mullan 2007
-
- Mullan F, Frehywot S. Non‐physician clinicians in 47 sub‐Saharan African countries. Lancet 2007;370(9605):2158‐65. - PubMed
Puri 2014
-
- Puri M, Tamang A, Shrestha P, Joshi D. The role of auxiliary nurse‐midwives and community health volunteers in expanding access to medical abortion in rural Nepal. Reproductive Health Matters 2014;Suppl (43):1–10. - PubMed
Renner 2012
-
- Renner RM, Brahmi D, Knapp N. Who can provide effective and safe termination of pregnancy care? A systematic review. BJOG 2013;120(1):23‐31. - PubMed
RevMan 2014 [Computer program]
-
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.3 . Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014 .
Samora 2007
-
- Samora JB, Leslie N. The role of advanced practice clinicians in the availability of abortion services in the United States. Journal of Obstetric, Gynecologic, and Neonatal Nursing 2007;36(7):471‐6. - PubMed
Sedgh 2012
-
- Sedgh G, Singh S, Shah IH, Ahman E, Henshaw SK, Bankole A. Induced abortion: incidence and trends worldwide from 1995 to 2008. Lancet 2012;379(9816):625‐32. - PubMed
Strauss 2005
-
- Strauss SE, Richardson WS, Glasziou P, Haynes RB. Evidence‐based Medicine: How to Practice and Teach EBM. 3rd Edition. Vol. 1, New York : Churchill Livingstone, 2005.
WHO 2008
-
- World Health Organi zation. Task shifting: rational redistribution of tasks among health workforce teams. Global recommendations and guidelines. WHO Press 2008.
WHO 2010
-
- World Health Organi zation. Mid‐level health providers a promising resource to achieve the health Millennium Development Goals. WHO Press 2010.
WHO 2012
-
- World Health Organization, Department of Reproductive Health and Research. Safe Abortion: Technical and Policy Guidance for Health Systems. 2nd Edition. Geneva: World Health Organization, 2012.
Yarnall 2009
-
- Yarnall J, Swica Y, Winikoff B. Non‐physician clinicians can safely provide first trimester medical abortion. Reproductive Health Matters 2009;17(33):61‐9. - PubMed
References to other published versions of this review
Barnard 2014
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous